
What is Laryngeal Cancer?
Laryngeal cancers, which are cancers found in the larynx (also known as the voice box), make up one-third of all head and neck cancers and are a significant cause of illness and death. They mostly start in one of three regions of the larynx: the area above the vocal cords (supraglottis), the vocal cords themselves (glottis), or the area below the vocal cords (subglottis), and each has its own system for measuring the severity or stage of cancer.
The most common type of laryngeal cancer is called squamous cell carcinoma. Other types, which are very rare, include sarcomas, minor salivary gland carcinomas, melanoma and lymphomas. Typically, people with a significant history of smoking are more likely to be diagnosed with laryngeal cancers. There is also a link between these cancers and alcohol consumption (supraglottis), Agent Orange, asbestos, metal-working fumes (all areas), and others.
Subglottic cancer, or cancer in the area below the vocal cords, is quite rare, and unfortunately, it usually has a poor outlook. Notably, the connection with the human papillomavirus (HPV) is not as strong as in some throat cancers. While certain HPV-related pathways have been identified in laryngeal cancers, we still need to understand their exact role and influence on the outcome of the disease.
The symptoms, how the cancer spreads, the outlook, and the treatment all depend on which part of the larynx the cancer originated. Early-stage (stage I or II) cancer in the supraglottis and glottis is often highly treatable or curable, although unfortunately the same is not true for the subglottis. Early-stage laryngeal cancer can often be successfully treated with a single type of treatment, either surgery or radiation therapy, which usually allows for the larynx to be preserved. However, for more advanced cancer (stage III or IV), the outlook is less certain for all areas, with the best outcomes often seen in glottic cancers followed by supraglottic and then subglottic tumors. Treating advanced-stage laryngeal cancer typically requires a combination of surgery, radiation therapy, and chemotherapy.
Everything mentioned so far specifically relates to squamous cell carcinoma of the larynx. Other types of cancer, such as minor salivary gland carcinoma, laryngeal melanoma, and other rare cancers, are mainly managed within clinical trials due to their rarity, which prevents standardized treatment recommendations. Sarcoma of the larynx, particularly chondrosarcoma (the common subtype), is usually treated surgically. Notably, though these cases are rare, their overall prognosis is often favorable, even though the treatment can require a total laryngectomy, complete removal of the larynx, which can have severe consequences.
What Causes Laryngeal Cancer?
Smoking is the biggest contributor to laryngeal cancer, also known as cancer of the voice box, being responsible for over 70% of all cases. People who have a history of smoking are at a greater risk, and current smokers face an even higher risk than those who have quit. Add to that, it’s also seen that smokers are more likely to get supraglottic cancers (cancer above the vocal cords) than glottic cancers (cancer on the vocal cords).
Heavy alcohol drinking is also linked to laryngeal cancer, though the exact impact is hard to determine because people often smoke and drink together. There’s also some evidence that marijuana smoking might be a risk factor in younger people.
A few other risk factors for laryngeal cancer include:
– Being exposed to second-hand smoke for a long time. If you’ve been exposed to second-hand smoke for more than 20,000 hours in your life, your chance of getting laryngeal cancer goes up.
– Being male, as men are 4-5 times more likely to get this type of cancer compared to women.
– Being White or Black. In North America, those two demographics have a noticeably higher rate of tobacco-related cancers compared to Asian-Americans and Hispanics.
– Genetic and other syndromes, like Fanconi anemia, Plummer-Vinson syndrome, and dyskeratosis congenita, can also increase the likelihood of developing laryngeal cancer.
Finally, being exposed to certain occupational and environmental factors, including Agent Orange, asbestos, nickel fumes, sulfuric acid mist, and wood dust, can also raise the risk of getting laryngeal cancer.
Risk Factors and Frequency for Laryngeal Cancer
In 2017, laryngeal cancer, a type of head and neck cancer, was the cause of 13,150 new cases and 3710 deaths. The average age of those affected is 65, and it is more common in males and Blacks. Interestingly, the number of new cases decreases by about 2% each year due to less people smoking.
The majority, about 98%, of laryngeal cancers start in either the supraglottic or glottic areas. Cancer of the glottic region is three times more common than that of the supraglottic region. Only a small percentage, about 2%, begin in the subglottic area. The good news is, if caught early, these cancers can often be cured. In fact, with early detection, there is a 90% to 95% success rate for controlling T1 glottic cancers, and a 80% to 90% success rate for early-stage supraglottic cancers. These early cases can usually be treated in a way that spares the vocal cords, meaning the patient can retain their voice after treatment.
However, more advanced cancers are more difficult to control, having a success rate of between 40% and 70%. If the cancer has grown large or spread (referred to as T4 disease), the best treatment is often removal of the larynx (laryngectomy). Although this is a major surgery, medical advancements have improved the process and patients can often regain their speech after the operation.
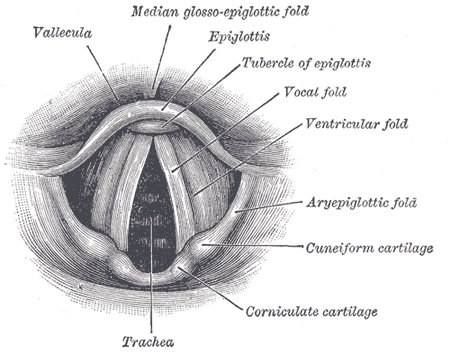
larynx, including the vallecula, epiglottis, tubercle of the epiglottis, vocal
fold, ventricular fold, aryepiglottic fold, cuneiform cartilage, corniculate
cartilage, and trachea.
Signs and Symptoms of Laryngeal Cancer
Laryngeal cancer, or cancer of the voice box, often affects men, particularly those with a history of smoking and chronic alcohol misuse. Early symptoms can include a hoarse voice, throat pain when swallowing, and referred ear pain, which all point to more advanced stages of the disease. For supraglottic cancer, the pain when swallowing appears first, followed by hoarseness, indicating a more advanced stage. Usually, cancer spreads or metastasizes to the lymph nodes in the neck, presenting as firm, painless lumps. Later symptoms across all areas of laryngeal cancer include weight loss, difficulty swallowing, coughing or choking on food, and difficulty breathing.
Identifying when the symptoms began and how long they’ve lasted, along with any factors that worsen or improve them, is important for a correct diagnosis. Other conditions like viral infections, reflux disease, and other upper respiratory tract diseases can have similar symptoms and are often mistaken for laryngeal cancer. While reflux disease was once thought to be a risk factor for this cancer, recent studies do not consistently support this.
However, comprehensive examinations of the head and neck, along with tests to visualize the upper part of the gastrointestinal tract, are necessary for screening those at risk. Population-based screening is not effective, but it seems that screening high-risk patients might be beneficial.
In a physical examination, doctors observe the suspected cancerous tissue using various methods like mirror laryngoscopy, direct laryngoscopy, or most commonly, fiberoptic endoscopy. The goal is to determine the tumor’s size, its extent, involvement with nearby structures, and assess the mobility of the vocal cords.
While doctors can gain information about the extent of the disease and collect tissue samples during a direct laryngoscopy, a thorough neck examination is also necessary to evaluate the spread of the disease to the lymph nodes and the primary tumor’s extension. However, these physical signs alone can lead to false-positive results, so imaging tests are vital for diagnosing a mass in the larynx. Tests to assess cranial nerve function are also crucial, as abnormalities may suggest the spread or severity of the disease.
Testing for Laryngeal Cancer
To diagnose and examine the stage of laryngeal cancer, apart from patient’s history, physical examination, and visual examination of the larynx (voice box), a few more tests are needed. A biopsy, which is a way to extract and examine tissues, can be obtained from the primary suspect region through a procedure known as direct laryngoscopy. Additionally, a technique called fine-needle aspiration cytology may be employed for gathering cells from suspected areas of around the neck, often known as nodal disease.
All laryngeal cancer cases require imaging of the primary cancer region and lymph nodes close by, typically via a contrast-enhanced computed tomography (CT) scan of the neck. This type of scan helps to visualize areas not easily viewable through direct laryngoscopy, such as the region below the vocal cords, front of the epiglottis (a flap in the throat that keeps food from entering the windpipe), inner wall of the thyroid cartilage, space around the larynx, and presence of cancer outside the lymph nodes. All of these are critical for accurately determining the cancer stage.
If the cancer appears to be advanced, a chest CT scan along with a PET/CT scan (positron emission tomography) may be done to confirm if the cancer has spread to other parts of the body. If there’s suspicion that the cancer might have spread to areas like the lower part of the throat or the cervical part of the esophagus (tube connecting the throat to the stomach), procedures like esophagogastroduodenoscopy (EGD – looking inside your esophagus, stomach and the first part of small intestine using a small, flexible tube), and/or a barium swallow (a test that allows your doctor to look at your esophagus) may be done to identify the exact location of cancer.
Additional blood tests are required before starting any definite treatment. These include tests to measure complete blood count, platelet count, function of liver and kidneys, blood type, thyroid function, electrolyte balance, and albumin levels.
A patient’s eligibility for surgery and the extent of the procedure required depends on different factors such as mobility of vocal cords, presence of cancer in the neck or at distant sites, cancer spread to the base of the tongue, paraglottic and pre-epiglottic spaces, thyroid cartilage, carotid artery and its coverings, esophagus, surrounding soft tissues and muscles, and neck lymph nodes.
Treatment Options for Laryngeal Cancer
The treatment approach for laryngeal (throat) cancer is determined by the stage of the disease and the location of the tumor at the time of treatment.
In early stages, which include stage I and II of the disease, these cancers can be effectively addressed either by using radiation therapy or through surgery. The choice to prefer one over the other often rests on the healthcare provider’s experience and the patient’s preference. For patients with cancer in the glottis (voice box), voice-saving surgery is an option, although it may be influenced by the patient’s condition and the shape and structure of the throat. On the other hand, for those whose condition is too complex to use endoscope-led techniques, radiation therapy proves a better option. This is mainly to avoid the risks related to surgical procedures in such cases.
Like glottic cancers, early-stage supraglottic cancers (located above the vocal cords) can also be managed using voice box preserving surgery or radiation therapy. However, due to the significant chance of cancer spread through lymph nodes, it becomes necessary to treat both sides of the neck in supraglottic cancers. For those in later stages of supraglottic cancers, surgery could include endoscopic resection (removal of cancerous tissue using an endoscope) or open surgery often followed by radiation therapy.
Advanced stages of throat cancers are more complex and often require multi-approach treatment involving surgery followed by radiation therapy or a combination of chemotherapy and radiation therapy. While surgery may not always result in preserving the larynx, chemotherapy along with radiation therapy can still keep it intact. For particularly advanced cases (T4 stage), surgery has been shown to provide similar control of the disease compared to chemotherapy combined with radiation therapy. However, surgery has shown improved overall survival rates.
In terms of post-operative measures, radiation therapy is typically used when advanced tumor and lymph node stages are found through surgical examination. It is also employed in the presence of certain high-risk features, such as when cancer cells are found close to the surgery margins, tumor spread in the nerve cells, or emergency windpipe insertion due to serious tumor invasion. Lesions in the lungs, liver, or bones are common places for throat cancer to spread. If such metastasis occurs, treatment becomes systemic involving chemotherapy and/or immunotherapy which is mainly used to relieve symptoms.
It’s important to note that squamous cell carcinoma makes up most throat malignancies. However, other rare tumors include minor salivary gland malignancies and connective tissue tumors, such as sarcomas and melanomas. The treatment for these less common cancers depends on their type, and often involves measures to ensure airway protection. Some cases may require major surgical procedures, including total laryngectomy (removal of the larynx), to control the cancer, even in the early stages.
What else can Laryngeal Cancer be?
When considering a diagnosis for laryngeal cancer, doctors need to think about other conditions that may cause similar symptoms and exclude them. These conditions include:
- Acute sialadenitis (inflammation of the saliva-producing glands)
- Reactive lymphadenitis (inflammation of the lymph nodes)
- Benign tumors (non-cancerous growths)
- Branchial cleft cyst (a type of birth defect in the neck)
- Fungal laryngitis (fungal infection of the larynx, or voice box)
- Chronic sialadenitis (long-term inflammation of the saliva-producing glands)
- Contact granuloma (growths on the vocal cords caused by voice misuse or overuse)
- Hemangioma (a benign tumor made up of blood vessels)
- Laryngeal papilloma (warts on the larynx or voice box)
- Laryngocele (an air-filled sac connected to the larynx)
- Vocal cord polyp (a blister-like growth on the vocal cords)
- Vocal cord nodule or singer’s nodule (a small, benign growth on the vocal cords)
- Reinke edema (swelling of the vocal cords)
- Thyroglossal duct cyst (a type of birth defect in the neck)
- Gastroesophageal reflux disease (GERD, a long-term condition where stomach acid comes up into the esophagus)
- Granulomatous disease such as Wegener granulomatosis (a rare disorder that causes inflammation of the blood vessels)
- Sarcoidosis (an inflammatory disease that can affect multiple organs)
- Laryngeal tuberculosis (TB infection of the larynx)
- Syphilis (a sexually transmitted infection)
Surgical Treatment of Laryngeal Cancer
Treatment for laryngeal cancer, which is cancer in your voice box, might involve three types of surgery: endoscopic or transoral surgery, open framework surgery (otherwise known as partial laryngectomy), and total laryngectomy.
Endoscopic or transoral surgeries are conducted through your mouth or with specific scopes that help doctors visualize your larynx. However, not everyone can have this surgery as it depends on how well your doctor can see the affected area. Endoscopic cordectomy, a type of endoscopic surgery typically performed with a specific laser or with micro-laryngeal instruments, involves removing the affected vocal fold. This type of surgery is usually for the initial, or T1, and selected T2, stage of cancer in the vocal cords.
Another type of endoscopic surgery called supraglottic laryngectomy is performed for cancers in the supraglottis, the upper part of the larynx, and can also be done using a laser or with the help of a robot. It’s crucial to take the patient’s lung function into account for this type of surgery as there can be a risk of inhaling small amounts of food or liquid into the lungs after the surgery, but the outcomes are generally favorable in the right candidates.
Open framework surgery or partial laryngectomy is used for T1, T2, and selected T3 cancers in the voice box. There, vertical partial laryngectomy is for cancers in the vocal cords. With this surgery, the entire affected vocal cord along with part of the thyroid cartilage is usually removed, although its use is becoming less common today due to the availability of endoscopic resection.
Supraglottic laryngectomy, another type of open surgery, involves removing all supraglottic structures, including the epiglottis, the upper part of the thyroid cartilage, the hyoid bone, and the false vocal folds. Supracricoid laryngectomy is another surgical option for T3 and selected T4 tumors that can’t be removed from the supraglottis because they involve the vocal folds. In this procedure, the thyroid cartilage, both false vocal folds, and the ipsilateral true cord and arytenoid are removed. The remaining larynx is then suspended to the hyoid bone or the epiglottis to maximize the swallowing function post-surgery.
Total laryngectomy involves removing all tissues from the tongue base to the superior trachea and creating a permanent hole or stoma in the front of your neck for breathing. This surgery is used in advanced stages of the disease or when the voice box has lost its function or in cases of recurrence after prior radiation therapy. After this surgery, you’ll be completely dependent on breathing through your neck and you’ll have a specific hole in your neck for that purpose. The reconstruction of the neopharynx, which connects your nose and mouth to your esophagus, depends on the extent of the tumor, and it might require using a regional or free flap for reconstruction.
What to expect with Laryngeal Cancer
The chances of recovering from laryngeal cancer, a type of throat cancer, largely depends on how advanced the disease is when treatment begins. Other factors such as the person’s overall health and whether or not they quit smoking can also influence this.
Generally, around 61% of people diagnosed with laryngeal cancer in the United States are likely to live for at least five more years. If the cancer is detected early and hasn’t spread beyond the vocal cords (larynx), this figure rises to 78%. However, if the cancer has spread to lymph nodes nearby (stage III), the five-year survival rate falls to 46%. If the cancer has spread to other parts of the body, the rate is 34%.
It’s worth mentioning that survival rates can vary depending on the specific area of the larynx where the cancer develops. Glottic cancer, which begins in the vocal cords, generally has the best outlook, while supraglottic and subglottic cancers, which start above and below the vocal cords respectively, have a lower survival rate.
The 5-year survival rate for glottic squamous cell carcinoma, a type of skin cancer that begins in the flat cells lining the surface of the larynx, is 77% overall. If detected and treated early (stages I and II), this can increase to 84%, but can fall to 52% if lymph nodes are affected, and 45% if the cancer has spread elsewhere.
The 5-year survival rate for supraglottic squamous cell carcinoma is overall 45%. If caught early, this can increase to 61%, but falls to 46% if there is lymph node involvement, and down to 30% if it has spread to distant sites.
For subglottic squamous cell carcinoma, the overall 5-year survival rate stands at 49%. If treated early, it can rise to 59%, but falls to 38% if lymph nodes are affected. Interestingly, if this type of cancer has spread distantly, the survival rate is 44%.
Possible Complications When Diagnosed with Laryngeal Cancer
The complications experienced from treating laryngeal cancer greatly depends on the treatment method used. Radiation therapy often leads to several side effects like difficulty in speaking, swallowing, and tasting. Other complications can include inflammation of the oral mucosa and skin, underactive thyroid, and continuous dry mouth. Surgical complications may vary based on the surgical procedure performed. This could lead to issues such as speech problems, complete loss of voice, swallowing difficulties, an abnormal connection between the pharynx and the skin, weakened shoulder muscles, bleeding, and risk of infection.
Common Side Effects:
- Difficulty in speaking (due to Radiation Therapy or Surgery)
- Difficulty in swallowing (due to Radiation Therapy or Surgery)
- Difficulty in tasting
- Inflammation of the oral mucosa (due to Radiation Therapy)
- Skin inflammation (due to Radiation Therapy)
- Underactive thyroid (due to Radiation Therapy)
- Continuous dry mouth (due to Radiation Therapy)
- Complete loss of voice (due to Surgery)
- Abnormal connection between the pharynx and the skin (due to Surgery)
- Weakened shoulder muscles (due to Surgery)
- Bleeding (due to Surgery)
- Risk of infection (due to Surgery)
Preventing Laryngeal Cancer
The best way to avoid getting laryngeal cancer, which affects your voice box, is by making healthy lifestyle choices and avoiding certain risks. The main cause of this type of cancer is smoking, so it’s crucial to quit if you smoke. Programs aimed at helping people quit smoking can dramatically lower the chances of getting this disease.
It’s also important to drink alcohol in moderation and avoid overexposure to harmful substances like asbestos or certain chemicals often found in factories and other industrial settings. These substances can increase the risk of laryngeal cancer.
Eating a diet filled with fruits and vegetables can also help. These foods are high in antioxidants and other beneficial nutrients that may provide some protection.
Education about the importance of regular screening can also help catch this type of cancer early. Detecting precancerous areas or tumors in their early stages can make treatment more successful.











