
What is Child Intussusception?
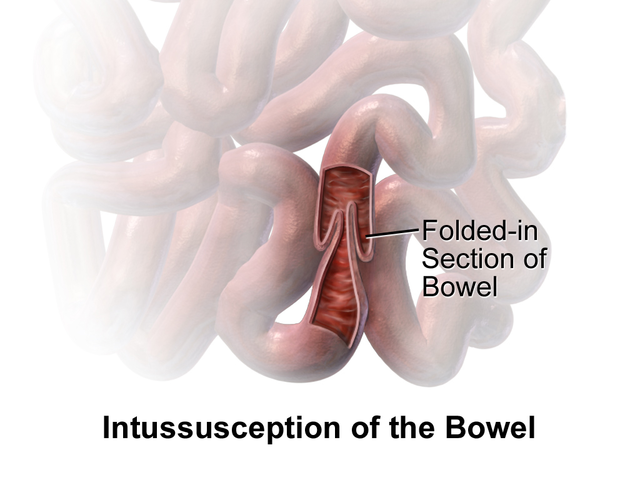
Intussusception is a condition where a part of the intestine slides into another section right next to it. This usually happens to the small intestine, but very rarely, also to the large intestine. Common symptoms of this condition are stomach pain, vomiting, swelling in the stomach, and passing bloody stools. Sometimes, it can even lead to a blockage in the small intestine. Other complications could include peritonitis, an inflammation of the lining of the abdomen, or a rupture in the bowel.
The cause of this condition is usually not known in children. However, in adults, it often occurs due to a tumor, which acts as a trigger point. Children with infections, cystic fibrosis, or polyps in their intestines are at a higher risk. In adults, the risk factors include the presence of endometriosis, adhesions in the bowel, and intestinal tumors. Doctors usually use medical imaging tests to diagnose this condition. In children, an ultrasound scan is often the preferred test, while in adults, a CT scan is commonly used.
Intussusception needs quick treatment. In children, the treatment usually involves an enema, which is a process of introducing fluids into the rectum and colon via the anus to expel its contents, with surgery being the next step if the enema doesn’t work. In adults, it’s often necessary to remove a part of the bowel. This condition is more common in children than in adults, especially in boys.
There’s an excessive incidence of intussusception during viral gastroenteritis seasons in some populations. Some forms of the rotavirus vaccine had led to a significant increase in instances of this condition, and so they had to be taken off the market. Ear infection, respiratory infection, and flu-like symptoms have been reported in about a third of the patients just before the onset of intussusception. Infections with adenoviruses can increase the risk of this condition. Interestingly, some patients who suffered from intussusception had a recent viral infection, either in the intestine or elsewhere in the body. In one study, adenovirus type C was identified as the biggest risk factor for intussusception. However, rotavirus infection and poliovirus vaccine were not linked to this condition. Another study found a connection between intussusception and human herpesvirus 6.
A rare type of this condition, known as pyloroduodenojejunal intussusception, occurs exceedingly rarely, especially in children. It occurs in around 10% of adult patients with intussusception. Known causes include polyps, Menetrier disease (a stomach disorder), hamartomas (benign tumor-like malformations), and gastrointestinal stromal tumors.
Bacterial infections, especially from bacteria like Salmonella, E. coli, Shigella, and Campylobacter, are also linked with this condition. The risk of intussusception usually increases in the first month after the infection.
While Intussusception can be serious, it’s not usually life-threatening. Diagnosis and treatment are often achieved with a barium, or an air-contrast enema, which is successful over 80% of the time. However, in about 10% of the cases, the condition may return within 24 hours.
What Causes Child Intussusception?
Intussusception is a condition whose precise causes remain largely unknown. This is particularly true for children, where about 90% of intussusception cases can’t be traced back to a specific cause. However, some suspected causes include infections, physical characteristics of the individual’s body (anatomical factors), and changes in how the intestines move food along (altered motility).
These identified causes could be:
* Infections
* Anatomical factors (specific physical traits or conditions)
* Altered motility (changes in the way your intestines move)
* Meckel’s diverticulum (a small pouch in the digestive system that one might be born with)
* Duplication (when a part of the body has its structure duplicated)
* Polyps (small, noncancerous growths)
* Appendicitis (inflammation of the appendix)
* Hyperplasia of Peyer patches (excessive growth of small areas in your intestines’ lining that help with immune functions)
* Idiopathic (medical term for causes that are unknown)
An obsolete version of the rotavirus vaccine, which is no longer in use, was once believed to cause intussusception. However, there seems to be no clear link between the current vaccines and this condition.
Risk Factors and Frequency for Child Intussusception
Intussusception is a medical condition that is typically diagnosed in infancy and early childhood.
- About 2000 infants in the United States are diagnosed with Intussusception in their first year of life.
- The condition usually appears around the fifth month, peaks from four to nine months, and then gradually decreases around the 18-month mark.
- Boys are more likely to be affected than girls, with a ratio of roughly 3 to 1.
- In adults, this medical condition accounts for 1% of cases involving bowel obstructions and is often associated with the development of abnormal growths like tumors.
Signs and Symptoms of Child Intussusception
Intussusception is a medical condition that affects the bowels. Its early signs include recurring stomach pain, feeling sick, vomiting a green liquid (because of bile), pulling the legs close to the chest, and stomach cramps. The pain comes and goes as the affected part of the bowel stops contracting from time to time.
As the condition progresses, you might see blood in the stool, which could look like “red currant jelly,” and a lethargic behavior. During a physical check-up, the doctor might feel a “sausage-shaped” lump in the abdomen. Children might start crying, pull their knees up to their chests, or have difficulty breathing due to pain spasms.
It’s important to note that fever isn’t a normal symptom of intussusception. However, if a loop of bowel becomes dead due to restricted blood flow (known as necrosis), it can lead to a hole (perforation) and sepsis, both of which cause fever.
In some rare instances, intussusception can be a complication of a condition known as Henoch-Schönlein purpura. Patients with this complication often experience severe stomach pain, along with the typical symptoms of Henoch-Schönlein purpura.
The symptoms of intussusception can be summarised as follows:
- Recurring stomach pain
- Feeling sick
- Vomiting a green liquid (because of bile)
- Pulling the legs close to the chest
- Stomach Cramps
- Blood in the stool, often like “red currant jelly”
- Lack of energy or lethargy
- A “sausage-shaped” lump in the abdomen
Testing for Child Intussusception
Intussusception, a condition in which a part of the intestine slides into the adjacent section, is usually identified through a thorough physical examination. One of the major signs doctors look for is known as the Dance sign. This involves observing the lower right part of the belly for any signs of retraction or pulling back, which could indicate intussusception.
A diagnosis can also be aided by a digital rectal examination. During this procedure, a doctor uses a gloved finger to detect any abnormalities in the rectum, and might be able to feel the intestine that has folded into itself (intussusceptum).
In some cases, however, additional imaging tests may be necessary for a definite diagnosis. Ultrasound, which uses sound waves to create a picture of the inside of your body, is the preferred diagnostic method for intussusception. Specific signs on ultrasound, such as the target or doughnut sign, can help confirm the diagnosis. This refers to the image seen on the scan, which appears like a 3cm large circular or doughnut shape. This doughnut shape is caused by the intestine and surrounding tissue appearing brighter (hyperechoic), encircled by the darker (hypoechoic), swollen outer layers of the bowel.
With another view, known as longitudinal imaging, the intussusception may even look similar to a sandwich.
A plain abdominal X-ray can also be useful, mainly to see if there’s any blockage in the intestine. Another procedure known as an air enema might be performed. This involves using air or a specific fluid to open up the intestine, which not only helps in diagnosing the condition but can sometimes even treat it by pushing the folded part of the intestine back into place.
In some situations, if the ultrasound results are unclear, a CT scan may be needed to confirm the diagnosis. Please note, this imaging test uses radiation and requires injecting a contrast material into your blood vessels. Therefore, it is less commonly used in young children as they may require anesthesia and there is a risk of exposure due to radiation and intravenous contrast.
Treatment Options for Child Intussusception
Intussusception — a condition where a part of the intestine slides, or “telescopes,” into another part — typically isn’t an immediate threat to life. It’s often treated successfully using either a barium, water-soluble, or air-contrast enema. This not only confirms the diagnosis, but also usually fixes the problem. This method is successful in more than 80% of cases. However, in about 10% of those cases, the problem may return within 24 hours.
If the intussusception can’t be fixed using these non-surgical methods, then surgery is required. During surgery, the doctor manually untangles the folded part of the intestine. If they aren’t able to unfold it, the affected section of the intestine is removed surgically. Intussusception can also be corrected through a procedure called laparoscopy, where special tools are used to pull apart the overlapping sections of the intestine.
What else can Child Intussusception be?
The possible conditions that can mimic some symptoms of appendicitis include:
- Abdominal hernias
- Blunt abdominal trauma in emergency medicine
- Colic
- Cycling vomiting syndrome
- Emergent treatment of gastroenteritis
- Gastric volvulus (a type of stomach obstruction)
- Internal hernia
- Testicular torsion
- Voluvulus, a condition that can lead to twist in the stomach or intestines
What to expect with Child Intussusception
Enema reduction is a medical procedure used to treat certain conditions, and many attempts have been made to improve its success rate using different compounds like glucagon and dexamethasone. Some promising results have been discovered when dexamethasone was added into the mix.
However, in the case of glucagon, there hasn’t been much evidence to show that adding it significantly increases the success rate of the procedure.
Possible Complications When Diagnosed with Child Intussusception
It’s important to treat intussusception (an intestinal disorder) as soon as possible to prevent complications. If left unaddressed, it may lead to serious problems such as gut rupture, tissue death in the intestines, and in rare cases, excessively short intestines. Post-operative intussusception – a rare complication – can also happen following certain surgeries like behind-the-abdomen tumor removal, Ladd procedure (surgery to correct twisted intestines), surgeries on the diaphragm, and pancreas removal. Up to 0.25% of children are at risk of experiencing this complication after undergoing a surgical procedure to open the abdominal cavity.
Common Complications:
- Gut rupture
- Tissue death in the intestines
- Excessively short intestines
- Post-operative intussusception
Surgeries with potential for Post-Operative Intussusception:
- Behind-the-abdomen tumor removal
- Ladd procedure
- Surgeries on the diaphragm
- Pancreas removal











