
What is Neonatal Hypertension?
Over the past four to five decades, doctors have started recognizing an issue known as neonatal hypertension, which is high blood pressure in newborn babies. At first, studying and managing this condition was difficult due to lack of equipment and data to measure a newborn’s blood pressure properly. Factors like how old the baby was when it was born, its current age, weight, and gender also made it tricky to define what is considered “normal” blood pressure for newborns.
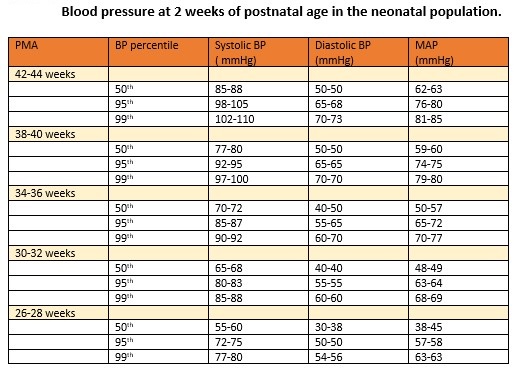
We still don’t fully understand the complete details of neonatal hypertension – how it develops, its long-term effects, and the best treatment methods. There is not enough agreement among medical experts about which medicine should be used to treat it. This condition is usually diagnosed when a newborn’s blood pressure is measured and found to be in the 95th percentile for the baby’s age, on three different occasions. A blood pressure value above the 99th percentile suggests severe hypertension and often requires immediate treatment and further investigation.
Doctors can measure a newborn’s blood pressure in two ways: invasive and non-invasive. The invasive method involves inserting a small catheter into an artery in the belly button, wrist, or back of the leg. The catheter is then connected to a device that monitors the baby’s blood pressure. However, this method is typically only used for very sick or premature babies, as it is complex and carries some risks.
The non-invasive method typically uses an automatic device that measures blood pressure based on the pulsations of the arterial blood flow. However, the readings from this device may sometimes be inaccurate and overestimate or underestimate the actual blood pressure. To avoid this, certain measures can be taken, such as making sure the cuff attached to the baby’s arm is the right size and that the pressure measurements are taken under optimal conditions (when the baby is calm and lying on their back, 1 to 1.5 hours after feeding). It’s also recommended to measure the blood pressure several times, with two-minute gaps in between and preferably on the right arm.
Though other non-invasive methods like using a traditional blood pressure gauge or ultrasound Doppler device are available, they are not commonly used in neonates. The former because the sounds made by blood flow are too faint to hear, and the latter because it tends to underestimate the blood pressure values.
What Causes Neonatal Hypertension?
Being born prematurely is a risk factor, and 75% of all newborns with high blood pressure are born early. These babies tend to have higher health risks, need longer stays in the Neonatal Intensive Care Unit (NICU), and are usually sicker. In newborns, the most frequent reasons for high blood pressure that needs medication are respiratory illnesses, certain drugs (like caffeine and dexamethasone), underdeveloped lungs (BPD), and kidney disorders.
Rarely, other factors can contribute to high blood pressure in newborns, including neurological issues like seizures, hormonal imbalances, heart conditions like coarctation of the aorta or Patent Ductus Arteriosus (PDA), and problems related to umbilical artery catheters.
Interestingly, having underdeveloped lungs (BPD) is a non-kidney-related risk factor for high blood pressure particularly in very low birth weight infants. Infants experiencing bleeding inside their brains may also risk developing high blood pressure. Rare causes include adrenal gland bleeding, vitamin D overdose resulting in kidney complications, and health issues due to long-term IV nutrition. Yet, the reason behind 57% of high blood pressure cases in newborns cannot be identified, and these are labeled as idiopathic or unexplained.
Risk Factors and Frequency for Neonatal Hypertension
Neonatal hypertension, or high blood pressure in newborns, varies in occurrence. In newborns that went full term, the rate is about 0.2%. This spikes up to 3% for newborns in the NICU, or Neonatal Intensive Care Unit. These rates can vary based on the group studied and how neonatal hypertension is defined in each study.
- About 1.4% of preterm infants need treatment for high blood pressure during their NICU stay, compared to 1% in full-term babies.
- The rate of neonatal hypertension in infants with Bronchopulmonary Dysplasia (BPD) is between 13% to 43%.
- The exact rate of neonatal hypertension in preterm babies is still unknown.
Signs and Symptoms of Neonatal Hypertension
Newborns that have neonatal hypertension (NH), often do not show symptoms and the high blood pressure is usually discovered during routine monitoring in the neonatal intensive care unit (NICU). Some may show symptoms like difficulty feeding, irritability, muscle too slack (hypotonia) or too tense (hypertonia), throwing up, struggling to breathe, low oxygen levels, and in severe cases, fast heart rate, heart failure, severe circulatory failure, and seizures. The symptoms can vary and are not specific. Usually, in older and full-term babies, this condition is found during routine checks in the NICU or during standard health check-ups after birth. Some babies who were sent home from the hospital might return with symptoms like irritability and poor weight gain.
A thorough physical examination is crucial. The overall appearance of the baby can indicate certain genetic conditions such as Turner, William’s, or Noonan syndromes, which are linked to a certain type of heart defect known as coarctation of the aorta. If there’s a difference in blood pressure and pulse between the arms and legs, it may suggest this heart defect. There can also be signs of heart failure like fast heart rate, unusual heart sounds, skin discoloration, and blueness due to lack of oxygen. Feeling the abdomen can reveal a lump which may indicate conditions like polycystic kidney disease, kidney tumors, swelling due to fluid build-up, and blood clots in the kidney veins. Checking the genitals may uncover birth defects or unclear physical sex traits in a condition called congenital adrenal hyperplasia. If there was a low amount of amniotic fluid during pregnancy (oligohydramnios), it might indicate birth defects of the kidneys, and in severe cases, the infant may be born with distinct features.
Testing for Neonatal Hypertension
In order to identify possible causes of neonatal hypertension (NH), which is high blood pressure in newborns, doctors begin with a detailed review of the mother’s and baby’s health history and perform a thorough physical examination. Considering that most cases of NH are often due to problems in the newborn’s blood vessels or kidney tissue, the first set of tests typically relate to these areas. These can include checking the levels of blood urea nitrogen, creatinine, electrolytes, and calcium in the blood, as well as analyzing the baby’s urine. It’s also important to test the urine for specific substances called vanillyl mandelic acid and homovanillic acid. An ultrasound that centers on the aorta and kidneys of the baby, using Doppler technology, also forms part of the initial examination.
Based on the findings from the health history review, physical examination, and initial tests, doctors may suggest further investigations. These could include tests to assess the functioning of the thyroid gland, cortisol levels, and the levels of aldosterone and renin activity in the plasma. Other tests may look at levels of plasma and urine catecholamines and metanephrines, serum 11 dexoycortisol, and 11 deoxycorticosterone. Tests may also be done for urinary 17-hydroxysteroid and 17-ketosteroid.
Additional evaluations could encompass a chest X-ray to check for bronchopulmonary dysplasia (BPD) or congestive heart failure, an echocardiogram or heart examination using ultrasound, and a voiding cystourethrogram, which investigates how well the baby’s bladder and urethra are functioning. Doctors might also suggest a captopril renal scintigraphy, which is a specific kind of kidney scan, and a dimercaptosuccinic acid renal scan to further examine the kidneys. A computed tomography (CT) scan may be done to thoroughly examine the renal artery and the aorta, along with an abdominal MRI, and an ultrasound of the head to rule out any issues like bleeding within the ventricles of the baby’s brain.
Treatment Options for Neonatal Hypertension
In most babies with neonatal hypertension (NH), addressing treatable causes can usually solve the problem. Anything that could be causing the issue, like an umbilical catheter, a high calcium level, or too much fluid intake, should be adjusted or removed. Some medication dosages might need to be reduced or stopped. Any surgical conditions should be treated if needed. Pain relief might also be given. If the baby has an endocrine disorder, specific hormone therapy should be provided. If high blood pressure continues to persist above the average despite these changes, blood pressure-lowering medicine should be started.
For mild high blood pressure: These babies can be checked regularly and watched closely. If the high blood pressure doesn’t go away on its own, it may be treated with a water pill (most recommended) or a different type of water pill.
For moderate high blood pressure: These babies have blood pressure readings between the 95th and 99th percentiles for their age with no signs of damage to important body parts. They can be treated with water pills (first choice), blood vessel relaxers, or heart rate and blood pressure lowering medicine. There is not much information on the indications and benefits of oral blood pressure-lowering medicines for mild to moderate high blood pressure in newborns.
For severe high blood pressure: If the blood pressure is greater than the 99 percentile, treatment with a continuous drip drug is warranted. A quick drop in blood pressure should be avoided. Monitoring blood pressure closely with a catheter directly in an artery is preferred in these patients.
Surgery might be necessary in treating newborn high blood pressure if certain conditions are present. These may include a narrowing of the aorta, blockage of the kidney artery or vein, blockage of the urinary tract or the place where the kidney and ureter connect, cystic kidney disease, neuroblastoma, or Wilms tumor, among others.
What else can Neonatal Hypertension be?
Neonatal hyperammonemia (NH) appears due to certain issues affecting various body systems. It’s important to investigate the root causes leading to NH. This condition can be tricky to identify as it presents common symptoms such as breathing difficulty, low muscle tone, fussiness, difficulty in feeding, and fast heart rate among others. These symptoms are also seen in numerous other newborn health problems. Hence, doctors need to ensure they’ve ruled out all these other potential causes through proper assessment and tests before confirming NH as the final diagnosis.
What to expect with Neonatal Hypertension
The outcome of Newborn Hypertension (NH) largely depends on the cause and severity of the condition. NH related to issues such as kidney blood clot, navel line insertion, or sudden damage to kidney tubes is often temporary and gets better as the original issue improves. If there’s damage to other organs, the prognosis is typically worse.
Most newborns usually need medication for a little while. Long-term treatment is rarely necessary. A study found that only 15 percent of infants discharged from hospital on blood pressure medication needed treatment by the age of 3 to 6 months.
Additionally, the progression of NH varies from hypertension in older children. A large study including 700 infants found that the average duration of treatment with blood pressure medications in the neonatal intensive care unit was ten days. Infants with high blood pressure due to Bronchopulmonary Dysplasia (BPD) usually have normal blood pressure at follow-up visits. However, NH due to kidney issues may persist into childhood and need long-term treatment.
Possible Complications When Diagnosed with Neonatal Hypertension
If babies with untreated severe high blood pressure are not treated, they may suffer damage to their major organs. This could lead to vascular injury, an enlarged left ventricle of the heart, brain disease, and high blood pressure-related vision problems. It’s crucial in such situations to get early and efficient treatment.
Frequent complications of chronic and severe high blood pressure can include high blood pressure-related kidney disease, which can vary in how it disrupts kidney function, and high blood pressure-related heart disease, which results in an enlarged or poorly functioning left ventricle of the heart.
The long-term negative effects and ongoing problems of untreated vs. treated high blood pressure in infants are not currently known. However, recent research evidence suggests that high blood pressure during childhood is linked with a high risk for high blood pressure in adulthood.
Preventing Neonatal Hypertension
High blood pressure in newborns often goes unnoticed in the nursery. It usually gets discovered during routine check-ups. It’s very important to catch and treat high blood pressure in infants quickly to avoid damage to their organs and long-term negative health effects. The problem is, giving medication for blood pressure to newborns can be hard as there haven’t been many studies on what works and is safe for them at this age. Plus, doctors aren’t sure what “normal” blood pressure should be for this group, which makes it even harder to treat.
There aren’t any set rules, especially about when to start blood pressure treatment or how to manage mild cases. Because most infants only need treatment for a short time (about 10 days on average) and many improve on their own over time, doctors should carefully consider the baby’s condition and other relevant factors before treating. For moderate high blood pressure, it’s usually suggested to start treatment with oral medication and introduce intravenous (IV) therapy if needed. In severe cases, starting oral treatment is recommended.











