
What is Recurrent Acute Rhinosinusitis?
Sinusitis, also known as rhinosinusitis, is a condition where the cavities around your nasal passages (sinuses) become inflamed. This inflammation can be caused by different things such as viruses, bacteria, fungi, and allergens. These causes often work together or one after the other to cause the inflammation.
In 1997, a group of experts, the Rhinosinusitis Task Force, came up with a list of major and minor symptoms to help doctors diagnose sinusitis. For a diagnosis of sinusitis, either two major symptoms or one major symptom along with two minor symptoms need to be present. The symptoms are as follows:
Major Symptoms:
- Nasal examination shows pus
- Nasal blockage
- Nasal discharge, pus, or discolored drainage from the nose
- A reduced ability to smell or complete loss of smell
- Fever
- Facial pain or pressure
- Feeling of congestion or fullness in the face
Minor Symptoms:
- Pain, pressure, or fullness in the ear
- Cough
- Toothache
- Fatigue
- Bad breath
- Fever
- Headache
Sinusitis can be classified into different types based on the duration of symptoms. Acute sinusitis lasts less than 4 weeks, subacute sinusitis lasts between 4 and 12 weeks, and chronic sinusitis lasts longer than 12 weeks. Recurrent acute rhinosinusitis (RARS) is a type where a person experiences 4 or more episodes of acute sinusitis in a year, with each episode lasting at least 10 days and no persistent symptoms between episodes. We will primarily discuss RARS, including how patients typically feel, how it is diagnosed, and how it is treated.
What Causes Recurrent Acute Rhinosinusitis?
The main causes of RARS, a type of sinusitis, are similar to those of other types of sinusitis. The most common cause is a viral infection in the upper respiratory tract, which is usually a temporary issue. In this case, the virus sets off inflammation and irritation in the nose and the surrounding sinuses. This inflammation can shrink the openings through which mucus and inhaled particles leave the sinuses, blocking the removal of these materials. Plus, inflammation can hinder the movements of tiny hairs called cilia, causing mucus to stay put and making the sinuses more likely to get a bacterial infection.
Like a viral infection, untreated hay fever can cause long-term inflammation in the nose and sinuses. This can obstruct the sinus outflow paths, build up secretions, and potentially cause a bacterial infection.
The most common bacterial species that cause RARS include Streptococcus pneumoniae, Haemophilus influenzae, other Streptococcus species, Moraxella catarrhalis, and Staphylococcus aureus. A drug-resistant bacteria called Methicillin-resistant Staphylococcus aureus (MRSA) often lives in the nostrils and can lead to repeated sinusitis episodes, especially in people who have taken several courses of antibiotics.
RARS and chronic rhinosinusitis share some common causes. For instance, noninvasive fungal pathogens like Aspergillus fumigatus might be present in these patients. Structural complications like enlarged turbinates, conchae bullosae, narrowed sinus openings, Haller cells, nasal polyps, nasal masses, and deviated septum, can make the nose and sinuses more prone to infection. These structural issues can often be fixed through endoscopic surgical techniques.
Genetic factors that affect nasociliary motion or mucus production, like Kartagener syndrome, are also thought to play a role in sinus disease. Other environmental factors, for instance, tobacco smoke and chronic exposure to inhaled irritants, can impact the disease’s development or severity. They do this by hindering ciliary movement and disrupting cell signaling in the body’s natural immune system, making the condition worse.
Risk Factors and Frequency for Recurrent Acute Rhinosinusitis
Sinusitis is one of the most frequently diagnosed health conditions. It’s so common that 1 in 8 adults will be diagnosed with sinusitis at least once in their lifetime. The condition is responsible for around 20% of all antibiotics prescribed. In 2015, there were 30 million diagnosed sinusitis cases in the United States alone, leading to treatment costs over $11 billion. Out of this total, $3 billion was spent on treating acute sinusitis and the rest on chronic sinusitis. A detailed look at medical insurance claims data from a six-year period (2003 – 2008) showed that 1 in 3000 people suffered from RARS. Most of these patients were female (around 72.1%), and the average age was about 43.5 years.
- Sinusitis is a common condition, with 1 in 8 adults receiving a diagnosis in their lifetime.
- It accounts for 20% of all antibiotic prescriptions.
- In 2015, there were 30 million diagnosed sinusitis cases in the United States, costing over $11 billion in treatment. -$3 billion was for acute sinusitis and $8.3 billion for chronic sinusitis.
- From 2003 to 2008, 1 in 3,000 people were found to have RARS in a review of medical insurance claims data.
- Most RARS patients were females, making up around 72.1% of cases, and the average age was 43.5 years.
- On average, these patients had 5.6 healthcare visits and filled 9.4 prescriptions per year, leading to an average annual cost of $1,091 per patient.
Signs and Symptoms of Recurrent Acute Rhinosinusitis
Acute sinusitis is a condition where people experience particular symptoms for less than four weeks. These symptoms can vary but generally include a runny or post-nose drippy nose, blocked nostrils, reduction or loss of smell, fever, facial or dental pain, tiredness, bad breath, and a headache. For people with recurrent acute sinusitis, they will experience at least four episodes of these symptoms within the previous year. Treatment often includes nasal sprays, steroids, and antibiotics.
- Runny or post-nose drippy nose
- Blocked nostrils
- Loss or reduction in smell
- Fever
- Facial or dental pain
- Tiredness
- Bad breath
- Headache
- Multiple episodes in a year for recurrent cases
During a physical check-up, doctors may notice things like a runny nose or throat drainage, swollen nasal structures, red or swollen nose lining. They may also find tenderness when touching the forehead or the cheeks. Some patients may have fever or rapid heartbeat due to facial pain. In rare cases, acute sinusitis can lead to more severe conditions like orbital cellulitis, preseptal cellulitis, or cavernous sinus thrombosis, so doctors will typically check the function of your facial nerves and the condition of your eye sockets to rule these out.
Patients with recurrent acute sinusitis often have symptoms similar to acute sinusitis. If the symptoms last less than ten days during an episode of sinusitis, it is usually caused by a virus. If symptoms persist for more than seven days or get worse within two days after initially getting better (known as “double worsening” or “second sickening”), it could be a sign of bacterial infection. The good news is most episodes of sinusitis, whether caused by a virus or bacteria, get better within 10-14 days.
Testing for Recurrent Acute Rhinosinusitis
To diagnose Recurrent Acute Rhinosinusitis (RARS), a medical condition that affects your nose and sinuses, doctors focus on your medical history and a physical examination. They’ll ask questions about your symptoms, how long you’ve had them, and how they’ve changed over time. This helps the doctors determine if your condition meets the diagnostic criteria defined by the American Academy of Otolaryngology-Head and Neck Surgery. In some cases, if your symptoms are severe, only affect one side, or don’t improve with treatment, your doctor might use a special tool called a nasal endoscope to look more closely at your sinuses.
Typically, doctors don’t order imaging tests like CT scans for simple cases of RARS. But, if you have chronic rhinosinusitis (long-term inflammation of the sinuses), suspected unusual physical features of your sinuses, or potential eye-related complications, a CT scan may be recommended. CT scans are also useful for planning surgeries like balloon sinuplasty and functional endoscopic sinus surgery (FESS), both of which can help treat sinus issues. Although, it’s worth noting that research suggests CT scans may be overused for patients with sinusitis.
When sinusitis is persistent or chronic, it may be necessary to take cultures (samples) from your sinuses to identify any bacteria or fungi that might be causing your symptoms. The most common culprits that cause RARS are the same ones that typically cause acute sinusitis, and include various types of bacteria such as S pneumoniae, H influenzae, M catarrhalis, S aureus, and other Streptococcus species.
Treatment Options for Recurrent Acute Rhinosinusitis
Managing recurrent acute rhinosinusitis, also known as RARS, usually involves a variety of treatments to address the different elements of the disease. Here are some of the common methods:
Nasal saline irrigation is useful in removing debris and potential harmful agents from the nose, providing some relief from symptoms. Different types of saline solutions can be used, with more salt-heavy solutions sometimes causing minor issues like increased nasal discharge and localized discomfort. It’s important to avoid excessive irrigation, which could disrupt the natural protective mechanisms in the nose and sinuses.
Topical corticosteroid nasal sprays are also used to reduce inflammation in the nasal tissues that can block sinus drainage. They’re useful not only in preventing the development of symptoms but also in managing acute infections.
Topical antihistamines like azelastine can also help reduce inflammation and irritation in nasal tissues, reducing swelling and opening up the sinus openings.
Topical decongestant sprays, such as oxymetazoline and phenylephrine, can help alleviate congestion through local narrowing of blood vessels. Prolonged use of these medications should be avoided to prevent rebound congestion, a side effect characterized by worsened congestion after the medication is stopped.
Antibiotics are used in the treatment of RARS, but should be cautiously used and typically only if symptom persists for more than a week or if symptoms become worse after initially improving.
Oral decongestants can help control symptoms such as inflammation and excessive secretions in the nasal, sinus, and respiratory tract membranes. These can assist in maintaining the patency of the nasal openings, thereby reducing sinus pressure.
Oral antihistamines interrupt the histamine pathway that leads to swelling and inflammation caused by allergens. These medications may be beneficial for patients whose sinus infection is thought to be triggered or worsened by allergic rhinitis.
Oral steroids, while not recommended as the primary therapy for acute rhinosinusitis, can be used alongside antibiotic therapy in some cases.
Modifiers of leukotriene, a substance involved in inflammation, such as montelukast, can be beneficial for patients with RARS who also suffer from asthma, allergic rhinitis, or nasal polyps.
If medical management does not produce sufficient results, surgery may be considered, especially for patients with documented anatomical abnormalities that may be contributing to their symptoms. Preoperative CT imaging is usually performed for surgical planning and to assist in locating the exact area to be addressed during surgery.
There are a couple of surgical interventions used, including functional endoscopic sinus surgery, designed to correct anatomical abnormalities that obstruct proper sinus drainage. Another option is balloon sinuplasty, which is a gentle method of permanently opening the sinus openings and drainage pathways to improve drainage of mucus and reduce pressure in the sinus cavities. This method is usually used in patients with RARS and chronic rhinosinusitis without nasal polyps.
Septoplasty, a surgical procedure for patients with deviations of the nasal septum that can block breathing, can also help improve sinus drainage. Similarly, reducing the size of the turbinates (small structures inside the nose) may help relieve nasal obstruction and support proper drainage of the nasal and sinus cavities.
What else can Recurrent Acute Rhinosinusitis be?
There are several diseases that share similar symptoms with RARS, hence the doctor needs to be careful in diagnosing it. Before coming to a conclusion, it’s crucial to ensure that the following conditions are not the actual cause:
- Allergic rhinosinusitis
- Acute rhinosinusitis
- Chronic rhinosinusitis with nasal polyps (CRSwNP)
- Chronic rhinosinusitis without nasal polyps (CRSsNP)
- Subacute rhinosinusitis
- Viral rhinosinusitis, typically related to upper respiratory tract infection
- Noninvasive fungal rhinosinusitis
- Invasive fungal rhinosinusitis
- Adenoiditis
- Cerebrospinal fluid leak in the nose (CSF rhinorrhea)
- Vasomotor rhinitis, a type of nonallergic rhinitis
- Reflux diseases, like laryngopharyngeal/gastroesophageal reflux disease
This is important in order to prevent misdiagnosis and to ensure that the most suitable treatment is prescribed.
What to expect with Recurrent Acute Rhinosinusitis
The outlook for patients suffering from recurring acute rhinosinusitis, a condition characterized by inflammation of the sinuses and nasal cavities, is generally positive. Most patients react well to treatment, which usually includes nasal sprays and oral antibiotics. It’s rare for individuals to develop severe complications that need emergency surgery or intravenous antibiotics, which are antibiotics given through the vein.
When surgery becomes necessary, patients typically report a considerable decrease in symptoms and a noticeable improvement in their quality of life. This shows the effectiveness of the medical approach in managing this condition.
Possible Complications When Diagnosed with Recurrent Acute Rhinosinusitis
While not common, repeated episodes of acute rhinosinusitis can lead to several complications including:
- Constant diminished or lost sense of smell
- Skin infection surrounding the nasal septum
- Infection of the eye socket
- A collection of puss between the skull and its outer covering
- Abscess in the eye socket
- Clotting in a large vein at the base of the brain
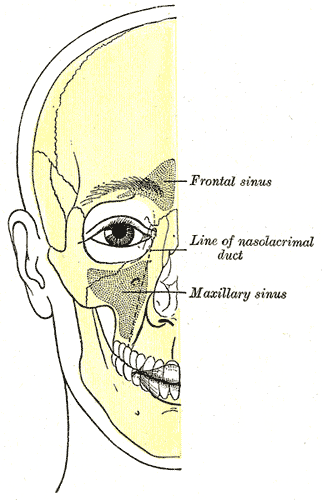
outline, highlighting the positions of air sinuses, including the frontal sinus,
line of the nasolacrimal duct, and the maxillary sinus.
Preventing Recurrent Acute Rhinosinusitis
Teaching patients about what to expect in terms of how their symptoms might progress, how they can manage symptoms at home, and when they should seek medical help is incredibly important. This kind of guidance helps patients to notice and deal with their symptoms earlier in the course of their illness. Effective early management of symptoms can help to prevent them from getting worse, which can mean that more serious and expensive treatments aren’t always necessary.
When additional treatment is needed, it’s also essential to educate patients about how their medicine should be taken, the common side effects that might occur, and what outcomes they can expect. This information can help patients to feel more satisfied with their care, and help them to understand their treatment.











