What is Peters Anomaly?
Peters anomaly is a rare eye disorder present from birth. It’s named after Dr. Alfred Peters, a German eye specialist, or ophthalmologist. This condition affects the front section of the eye and is recognized by a cloudy area on the center of the cornea (the clear outer layer of the eye). This cloudy area can differ in size and is caused by a defect that also affects layers beneath the cornea. Although the central cornea can be opaque, the outside part is generally clear. However, this cloudiness may spread to varying degrees from the center.
In Peters anomaly, some tissues called iridocorneal adhesions, which usually begin from the collarette (the thickest part of the iris), get bonded to the edges of the cloudy cornea. These adhesions can appear as tiny threads, thick strips or curved sheets.
In 1974, Townsend and his colleagues classified Peters anomaly into three types: Type I affects only the cornea and shows as a central irregularity; Type II shows an abnormal connection between the cornea and the lens with clouding of the cornea; and Type III shows a central corneal irregularity as well as a condition called Rieger mesodermal dysgenesis. Nowadays, Peters anomaly is grouped into two types.
Type I has the cloudy cornea together with the iridocorneal adhesion and it usually happens in one eye. The cloudiness of the cornea can be mild or severe, but the outer cornea is usually clear. Sometimes, there can be fluid build-up or change of the terminal part of cornea, which makes it look like the white part of the eye. Type I has less visual and systemic issues compared to Type II and it has a better chance of retaining vision. Type II features abnormal contact between cornea and lens or corneal cloudiness with lens imperfections. In Type II, the problem is usually found in both eyes and the lens is generally cataractous (cloudy) and stuck to the cloudy part of the cornea.
Those with Type II have a higher likelihood to have problems in other parts of the body. Peters-Plus syndrome is a term that was first proposed in 1984 and is used when Peters anomaly is noticed together with other systemic issues like cleft lip/palate, shorter-than-average height, unusual ears, and intellectual disability. Krause-Kivlin syndrome is a condition inherited in an autosomal recessive manner, which means both copies of the gene in each cell have mutations, that features Peters anomaly along with facial abnormalities, short stature disproportionate to body size, and slower than normal bone development.
What Causes Peters Anomaly?
Peters anomaly is a disorder that often occurs randomly, but it can sometimes be passed down through families. Research has shown that changes in certain genes like PAX6, PITX2, PITX3, COL4A1, FOXC1, and COL6A3 can cause this anomaly. The genes PAX6 and FOXC1 are commonly linked to Peters anomaly. One study found that in 20% of Peters anomaly cases, there was a mutation in a gene called CYP1B1. Other factors such as exposure to harmful substances during pregnancy, certain infections during pregnancy, and maternal alcoholism can also cause Peters anomaly.
PAX6
This gene is found on chromosome 11p13. It produces a protein that helps in the development of eye tissue and the central nervous system. The mutation of this gene can lead to various eye anomalies like aniridia (absence of the colored part of the eye), Peters anomaly, congenital cataract (clouding of the eye lens from birth), foveal hypoplasia (underdevelopment of the center of the retina), and optic nerve hypoplasia (underdevelopment of the optic nerve).
FOXC1
This gene, found on chromosome 6p25, plays a role in our body’s development. When this gene is altered or deleted, it could lead to defects in the eye, heart, and hearing. It has been linked to disorders of the eye’s anterior segment (the front part of the eye) and a condition called Axenfeld-Rieger syndrome type 3.
PITX2
This gene is located on chromosome 4q25 and helps with the development of the body. Mutations or deletions of this gene lead to eye, heart, and hearing defects. It’s estimated to be responsible for 40% of cases of Axenfeld-Rieger syndrome (an eye condition that could affect other body parts). Disorders linked to mutation in PITX2 include Axenfeld-Rieger syndrome, anterior segment dysgenesis 4, and ring dermoid of the cornea (a benign tumor in the cornea).
CYP1B1
This gene, located on chromosome 2p22.2, is linked to 20% of cases of Peters anomaly due to mutation.
TFAP2A
Located on chromosome 6p24.3, this gene is essential for the normal development of the lens, optic cup (part of the retina in the eye), and facial region. Mutation of this gene leads to branchiooculofacial syndrome (a condition that causes skin, eye, and cranial bone abnormalities).
COL6A3
Located at chromosome 2q37.3, this gene is crucial for collagen’s strength, a protein that gives structure to tissues and organs. There’s an abundance of collagen in the cornea (the eye’s front surface). Mutation of this gene can cause problems in the processing of proteins within cells, leading to a reduction in cellular resistance to stress. This gene’s mutation may be observed in cases with isolated Peters anomaly (an eye disorder that affects the cornea and the iris).
CHD2
This gene, situated on chromosome 15q26.1, helps cells adhere to each other. It’s found in developing parts of the eye, such as the lens stalk and the corneal endothelium, which is the layer of the cells on the inner surface of the cornea.
DOP1B
Found on chromosome 21q22, this gene helps proteins interact with each other. It has been linked to Peters anomaly in instances where family members intermarry.
B3GLCT
This gene, found on chromosome 13q12.3, controls the glucose transfer to a specific type of protein. When this gene is mutated, it leads to Peters plus syndrome, which is a genetic disorder characterized by the combination of Peters anomaly and other systemic abnormalities.
Other genes that are linked to Peters anomaly include PITX3, FOXE3, FLNA, HCCS, NDP, SLC4A11, and COL4A1.
Risk Factors and Frequency for Peters Anomaly
Peters anomaly, which is a type of malformation in the eyes, affects a significant percentage of newborns suffering from ocular malformations. Every year in the United States, there are 44 to 60 reported cases of Peters anomaly. In most cases, both eyes are affected but not in the same way. About half of the patients with Peters anomaly also have other issues with their eyes, and nearly 60% also have abnormalities elsewhere in their body.
- Between 3.3 and 6.0 out of 10,000 newborns have ocular malformations, with a majority being Peters anomaly.
- Every year, the US reports between 44 and 60 new cases of Peters anomaly.
- In the majority of these cases (80%), both eyes are affected, but differently.
- About 50% of patients with Peters anomaly also have other eye defects.
- Almost 60% of these patients also have abnormalities in other parts of their body.
Signs and Symptoms of Peters Anomaly
When checking a patient’s eyes for Peters anomaly, doctors might first discuss with the family how long the patient’s vision has been affected, how it’s progressed, if the mother had any exposure to harmful substances (teratogens), alcohol, or infections during pregnancy, and they also might examine the eyes of immediate family members for cloudiness in the center of the cornea (central corneal opacity).
This eye condition is often first spotted by pediatricians who note a blurring in the center of the cornea with an abnormal eye reflection. This blurry zone can have varying thickness and size, but the outer edge of the cornea usually remains clear. If it’s a type II Peters anomaly, there can be a blurry cornea, corneal attachment to the iris (iridocorneal adhesion), and lens abnormalities like cataracts. This condition can affect both eyes, increasing the risk of strabismus (crossed or misaligned eyes).
Those with Peters anomaly can also have eye fluttering (nystagmus), small cornea size (microcornea), flat cornea (cornea plana), and glaucoma due to malformed angle. Other eye issues can include iris abnormalities, tearing in the retina or choroid layer of the eye (retinal and chorioretinal coloboma), defective formation of the retina (retinal dysplasia), abnormal tissue in the eye (persistent hyperplastic primary vitreous), underdeveloped optic nerve (optic nerve hypoplasia), and drooping of the eyelid (ptosis).
- 50 to 70% of people with Peters anomaly can also have congenital glaucoma.
- Increased pressure inside the eye due to incorrect development of the eye’s drainage system.
- Though congenital glaucoma usually appears within the first year of life, it can show up later in childhood or even later.
Screening for bodily defects is also key. Abnormalities like developmental delay, seizure disorder, brain abnormalities, facial deformities such as cleft lip, heart defect, and abnormal bone structure might also be linked. Rare associations like Wilms tumor and linear skin defects could also appear with Peters anomaly. Abnormal corpus callosum and cortical development are often spotted in brain scans of patients with Peters anomaly. In a few cases, underdevelopment of the cerebellum, brain calcification, and incorrect formation of the hippocampus can present with the Peters anomaly. Bilateral cases of Peters anomaly have a higher chance (71.8%) of bodily abnormalities than unilateral cases.
Testing for Peters Anomaly
Peters anomaly is a condition that’s diagnosed through a clinical examination, often supported by some further tests to better understand the details and document any issues with the eyes.
Various Eye Tests
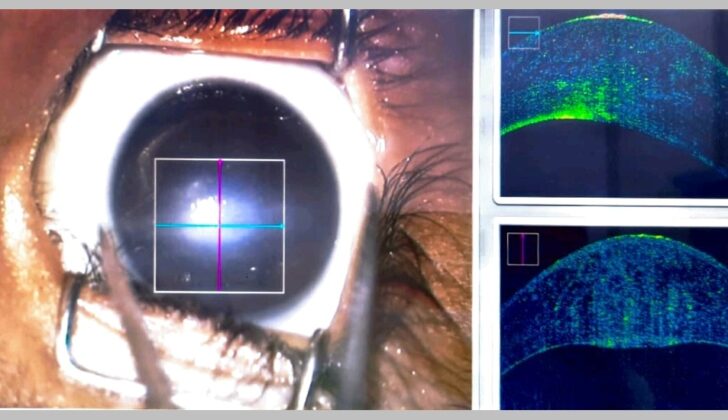
A photo of the front part of the eye (the anterior segment) can be very helpful. This image can be used to measure the size, shape, and location of the affected area, compare the condition of both eyes, and to explain the condition to you and your family. It’s also useful for comparing images before and after treatment, for remote consultations, and for research purposes.
A type of ultrasound scan called a B scan can provide more valuable information about Peters anomaly. This scan can highlight issues not visible to the naked eye, like a detached retina or a mass at the back of the eye.
Ultrasound biomicroscopy (UBM) is another non-invasive test for Peters anomaly. This device uses high-frequency sound waves that provide a detailed picture of the eye, which can show abnormalities that may not be visible in other types of tests. For example, UBM can detect a shallow front part of the eye, adhesion (the sticking together) of the iris and cornea, and early swelling of the cornea. It can also show if the Descemet membrane, a thin layer of the cornea, is missing.
Intraoperative OCT (iOCT, SD-OCT) is another advanced imaging technique. It generates detailed images of the eye, and can help surgeons to make decisions during eye surgery. This test classifies Peters anomaly into mild, moderate and severe categories, based on the specific eye abnormalities identified.
Close Examination of Eye Tissue
Sometimes, if the cornea (the clear front surface of the eye) is very cloudy or opaque, an examination of the tissue under a microscope might be needed. This can show changes in every layer of the cornea.
Imaging Beyond the Eye
In certain cases, a type of scan called an MRI (magnetic resonance imaging) might be needed to rule out problems in the brain or optic nerve that could be related to Peters anomaly. This type of scan can also help to differentiate between a long eye axis due to a defect in the eye, glaucoma, and nearsightedness.
Other Systemic Tests
Your doctors might also order other tests to examine the rest of your body. These could include an ultrasound scan of your heart to look for congenital heart disease, and an ultrasound of your abdomen to check for any abnormal development of the kidneys. They may also recommend a CT scan (computed tomography) of the brain to rule out any cerebral and ocular involvement.
Treatment Options for Peters Anomaly
For patients with Peters anomaly, the main aim of treatment is to improve eyesight and prevent any further loss of vision. This can be achieved through medical treatments or surgical procedures.
For the medical management of Peters anomaly, occlusion therapy is commonly used, especially in mild cases, to help prevent further vision loss. This method can be beneficial when the cloudiness in the cornea isn’t too dense, allowing some visibility of the back of the eye, in cases where the cloudiness affects only one eye, and in scenarios where the severity of cloudiness varies in both eyes.
It’s also important to control the pressure inside the eye before and after any surgery for glaucoma, a condition that is often seen in patients with Peters anomaly. However, medical treatments are not considered the ultimate solution for Peters anomaly.
Surgical procedures are generally the most effective treatment for Peters anomaly. However, the decision to perform surgery, especially at an early age, is dependent on various considerations. These can include the density of cornea cloudiness, the health of the lens, and any other eye abnormalities present.
There are several possible surgeries. One option is a procedure called peripheral iridectomy, which is typically used in cases where the cloudiness is limited to a specific area of the cornea with a clear margin and the lens is transparent. This surgery is considered safer and requires less aftercare. Another surgical option is penetrating keratoplasty combined with cataract extraction, commonly used when the lens is also abnormal or affected.
This penetrating keratoplasty surgery might be necessary in cases where the pupil is blocked by the cloudy cornea even after being dilated, the cloudiness in the cornea is particularly dense or when both eyes have dense cloudiness. One notable study found that this type of surgery was performed in approximately 65% of infant Peters anomaly cases. However, the success rate dropped to about 30% after 5 to 10 years following the surgery.
Factors that increase the risk of failure of corneal transplantation include the size of the graft, the presence of abnormal tissue growth inside the eye, the existence of central nervous system abnormalities, young age, and other associated congenital eye defects.
In some severe cases, an artificial cornea may be considered. However, this intervention generally has a poor outlook due to complications like glaucoma, inflammation of the eye tissues, and detachment of the retina.
Finally, glaucoma surgery, including procedures known as trabeculectomy, diode laser cyclophotocoagulation, trabeculectomy with mitomycin C, and implanting a glaucoma drainage device, may be conducted. These treatments help control the intraocular pressure, but additional medical management might also be necessary following surgery.
What else can Peters Anomaly be?
When a newborn has a clouded, opaque cornea, doctors must consider several conditions that may cause this. An easy way to remember these conditions is with the acronym STUMPED. This stands for:
- Sclerocornea: A rare disorder where the cornea becomes a bit like the sclera (the white part of the eye). The cornea may lose its clearness, especially at the edges, and other eye parts may be malformed too.
- Tear in Descemet Membrane: This can happen when forceps are used to assist in the delivery of a baby, causing clouding in the cornea. Long-term, this can cause astigmatism, and it may need treatment to correct the vision.
- Amniocentesis injury: A very rare condition where the cornea becomes cloudy due to a needle perforation. It can cause rise of intraocular pressure, eye deformities and cataracts.
- Ulcers/Keratitis: In newborns, viral infections like herpes or bacterial infections can cause corneal opacities. Though extremely rare, conditions like congenital rubella may also cause the cornea to become opaque during the first trimester of pregnancy.
- Mucopolysaccharidosis: An inherited disorder that causes cloudy corneas in the first year of life due to accumulation of a substance called glycosaminoglycans. Other eye issues may also be present.
- Other metabolic disorders: These can also cause corneal opacity. They include conditions like cystinosis, where cystine crystals are deposited in the cornea, and mucolipidosis IV, a rare metabolic disorder causing corneal opacity and other health problems.
- Endothelial Dystrophy: A hereditary condition that causes a constant fluid buildup in the cornea, making it less clear. This disease variates in severity.
- Dermoid: A choristoma (normal tissue in the wrong place) that mainly affects the epibulbar part of the eye, but occasionally the cornea.
In addition, congenital glaucoma may result in a hazy cornea with increased intraocular pressure. Other conditions like Posterior polymorphous corneal dystrophy, where the inside back of the cornea behaves like the outer layer, and Posterior Keratoconus, where the rear curvature of the cornea bulges out, may also need to be considered.
What to expect with Peters Anomaly
Your health outcome can depend on various factors such as your age, how severe the illness is, and any other medical conditions you may have. An early surgery, like penetrating keratoplasty (which is a corneal transplant), might prevent weak or blurry vision. However, it’s important to note that this surgery comes with a high chance of the transplanted cornea not surviving. A study conducted in 2005 revealed that only 22% of patients had clear transplants two years after the surgery.
Different types of the disease can also affect your prognosis. For example, Type I usually has better sight outcomes than Type II.
Possible Complications When Diagnosed with Peters Anomaly
Most complications that may occur with Peters anomaly arise following a type of cornea transplant known as penetrating keratoplasty. These post-surgery issues can include the failure of the graft (donor’s cornea), glaucoma (a group of eye diseases causing optic nerve damage), cataract (clouding of the eye’s lens), retinal detachment (emergency condition where the retina pulls away from the back of the eye), and phthisis (shrinkage of the eye). Glaucoma is the most frequent issue encountered after surgery. Complications are likely to occur in cases with larger grafts, multiple surgeries such as lens removal (lensectomy), removal of the eye’s vitreous (vitrectomy), and alongside corneal transplants. Complications that can occur outside of surgical interventions include “lazy eye” (amblyopia), rapid, uncontrolled eye movement (nystagmus), and crossed eyes (squint).
Following are the complications that may be encountered:
- Failure of the graft
- Glaucoma
- Cataract
- Retinal detachment
- Phthisis
- Amblyopia or ‘lazy eye’
- Nystagmus
- Crossed eyes or squint
Preventing Peters Anomaly
If your child is diagnosed with Peters anomaly, it’s important to have a genetic counseling and evaluation. This will help understand the cause and consequences of this condition. It’s crucial that doctors clearly communicate what this condition means for the child’s future health. Regular medical check-ups are very important. Parents and patients should also be taught about why it’s crucial to follow the treatment plan strictly. This is because children with Peters anomaly are at a higher risk of developing certain eye conditions like lazy eye (amblyopia), glaucoma, squint, among others.











