What is Volvulus?
Volvulus is a condition where a part of the intestine twists on itself and its supporting tissue, leading to a blockage in the bowel. This twisting can be gradual or sudden, and symptoms include abdominal swelling, pain, vomiting, constipation, and passing blood in stool. In severe cases, the twisting can disrupt the blood flow, which can damage the bowel and cause intense pain and fever.
There are a number of factors that can increase the risk of developing volvulus, such as abnormal rotation of the intestine, Hirschsprung disease (a condition present from birth that affects bowel movement), an enlarged colon, pregnancy, and abdominal adhesions (scar tissue). In addition, certain neurological conditions, such as Parkinson’s disease and multiple sclerosis, or physical issues like chronic constipation requiring regular laxative use, and certain muscle diseases can also increase the risk. In adults, the sigmoid colon and cecum (a pouch at the beginning of the large intestine) are most often involved, while in children, the small intestine and stomach are more likely to be affected.
To diagnose volvulus, doctors mostly rely on the patient’s symptoms but may also use imaging techniques like X-rays, ultrasound, or a type of X-ray that uses a dye to highlight the digestive tract. This topic mainly discusses volvulus in adults, and while children can also have a type of volvulus (midgut volvulus), it is beyond the scope of this simplification.
For treatment, specialists can try a procedure that involves inserting a tube via the rectum (sigmoidoscopy) or use of a specific fluid (barium enema) to untwist the bowel. However, the chance of the problem happening again is quite high, so doctors usually recommend an operation to remove the affected part of the bowel within two days. In severe cases where the bowel is excessively twisted or the blood supply is cut off, emergency surgery is necessary. For cecal volvulus, the unhealthy portion of the bowel is typically removed and if the cecum is still healthy, it can be put back and stitched in place. Yet, the risk of the condition returning is pretty high with conservative treatment alone.
What Causes Volvulus?
Volvulus is a condition that can happen when there are issues with the digestive system like an enlarged colon, an overly flexible support tissue in the intestines (called a “long mesentery”), a disease called Hirchsprung’s, pregnancy, abdominal adhesions (scar tissue), and chronic constipation. In adults, the most commonly affected part is the sigmoid colon (the last part of the colon), followed by the cecum (the beginning of the large intestine). In children, the small intestines are more commonly involved.
In most cases, sigmoid volvulus occurs due to an acquired condition. But cecal volvulus can develop because of an unusually flexible support tissue in the right side of the colon or cecum, or if the cecum is longer than it should be. People with severe neurological conditions, like multiple sclerosis or Parkinson’s disease or those taking certain medications for mental illnesses, are more prone to get sigmoid volvulus.
People who stay in nursing homes, particularly those who are bedridden and suffer from chronic constipation, have a higher risk of developing this condition. Volvulus is also more common in patients with muscle diseases such as Duchene muscular dystrophy or visceral myopathy.
In developing countries, a diet high in fiber can cause the sigmoid colon to become overloaded and twist around its supportive tissue. Also, diseases that cause the colon to enlarge, like Chagas disease or megacolon, can increase the risk of having sigmoid volvulus. In some rare cases, appendicitis or surgery may result in the formation of excessive scar tissue leading to volvulus.
Risk Factors and Frequency for Volvulus
Colonic volvulus, a type of bowel obstruction, made up about 2% of all bowel obstruction cases in the United States from 2002 to 2010. One subtype, sigmoid volvulus, accounted for 8% of all intestinal obstructions and typically occurs between the ages of 30 and 70. It’s more common in older men, African Americans, people with chronic constipation, and those with neuropsychiatric disorders.
Cecal volvulus, on the other hand, is more common in younger women. A different variant, midgut volvulus, most often appears in babies who have abnormalities in the positioning of their intestine. Volvulus in other parts of the gut can happen at any age and typically results from unusual intestinal contents or internal scar tissue, which is known as adhesions.
- Colonic volvulus was 2% of bowel obstruction cases in the U.S. between 2002-2010.
- Sigmoid volvulus, which is a subtype, accounted for 8% of all gut obstructions. It usually happens between the ages of 30 and 70.
- Sigmoid volvulus is more often seen in older men, African Americans, individuals with chronic constipation, and those with neuropsychiatric disorders.
- Cecal volvulus is more frequent in younger women.
- Midgut volvulus typically affects babies with abnormalities in their intestine’s position.
- Volvulus in other parts of the intestine can occur in people of any age, usually due to unusual intestinal contents or adhesions.
Signs and Symptoms of Volvulus
Sigmoid volvulus generally affects older men who have chronic constipation. The symptoms can start suddenly but may come on gradually in about one-third of patients. The symptoms of this condition include abdominal pain, a bloated belly, vomiting, constipation, bloody stool, unwillingness to eat, and fever. When patients with severe belly bloating show up at the hospital after a long delay, they often have widespread tenderness, guarding, and stiffness, indicating a more serious condition known as perforation peritonitis. This can also lead to unstable blood flow and issues with breathing.
On the other hand, newborns with a condition called midgut volvulus often show symptoms of vomiting of green bile, swollen upper abdomen, bloody stools, and an inability to be soothed. Older children with midgut volvulus may experience periodic abdominal pain, diarrhea, and poor growth.
- Abdominal pain
- Swollen belly
- Vomiting
- Constipation
- Bloody stool
- Loss of appetite
- Fever
- Widespread tenderness, guarding, and stiffness in severe cases
- Unstable blood flow and breathing issues in severe cases
- Newborn symptoms: vomiting of green bile, swollen upper abdomen, bloody stools, and unsoothability
- Older child symptoms: periodic abdominal pain, diarrhea, and poor growth
Testing for Volvulus
Diagnosing a condition called colonic volvulus (a twist in the large intestine) is primarily based on a doctor’s examination and the patient’s symptoms. However, due to potential overlaps in symptoms with other diseases, additional diagnostic tests such as radiology images are often needed.
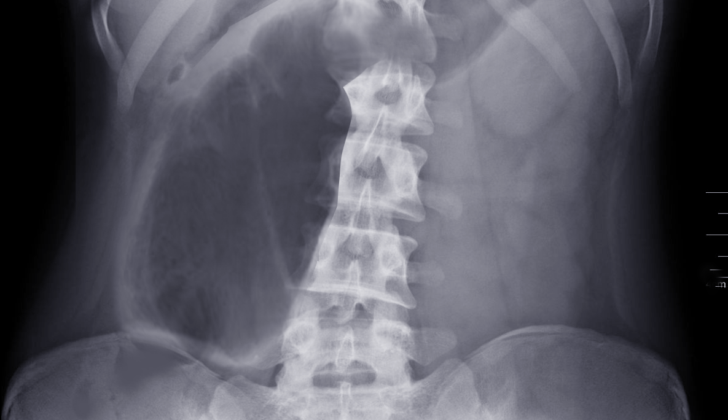
The initial investigation typically involves a simple X-ray of the abdomen. Certain signs on this X-ray, such as a “bent inner tube” or a “coffee bean,” are characteristic of a specific type of colonic volvulus called sigmoid volvulus. These signs describe how the twisted segment of the colon, which is filled with air, appears in the X-ray image, showing a thick inner wall and a thin outer wall. Likewise, for another type of volvulus called cecal volvulus, the X-ray may show an expanded small and large intestine.
A special X-ray test using a contrast agent (a dye that improves image clarity), known as a contrast enema, can also be done. However, this is only performed once the doctors are certain there is no perforation peritonitis – a severe condition where a hole develops in the bowel leading to inflammation in the lining of the abdomen. The contrast enema may show a “bird’s beak” formation, which is a characteristic sign of sigmoid volvulus.
A computed tomography (CT) scan, which is a type of X-ray that provides more detailed images, is generally not required for patients with a colonic volvulus. However, if performed, it may show a displacement of the appendix upwards along with blockage in the small and large bowel, which can indicate cecal volvulus.
For children suffering from a specific form of volvulus called a midgut volvulus, the X-ray may show fewer gas-filled areas in the intestine along with some scattered levels of air-fluid. An additional test called an upper GI series might show placement of a specific part of the small bowel called the duodenojejunal junction entirely to the right side of the abdomen.
Blood tests including a complete blood count (CBC) and tests for levels of chemicals in the blood can also be conducted. These tests, however, often show similar results in many medical conditions, so they’re not always indicative of a specific diagnosis.
Treatment Options for Volvulus
If you’re diagnosed with volvulus, a medical condition where part of the intestine twists around itself, doctors will ensure your body is stabilized before surgical treatment. This process, known as resuscitation, often involves broad-spectrum antibiotics, which fight a wide range of bacteria. Healthcare providers will also check your vital signs, such as blood pressure and heart rate, periodically and measure your urine output. They may position you on your left side to avoid pressure on a major blood vessel in your body called the vena cava.
The preliminary treatment for a particular type of volvulus, called sigmoid volvulus, starts with sigmoidoscopy, a procedure where a doctor inspects the lowest part of your large intestine using a thin, flexible tube with a camera. This procedure helps to both diagnose and initiate treatment for sigmoid volvulus. The doctor gently inserts the endoscope, the medical term for the flexible tube, and inflates the twisted part of your intestine with air. This attempts to untwist, or detorse, the portion of the intestine and reduce the blockage caused by the volvulus. This can be successful in between 50-100% of cases. Afterward, the doctor leaves a tube in place to discourage the intestine from re-twisting too soon.
However, since volvulus tends to occur again after this procedure, a surgery to remove that portion of the intestine usually happens within two days. If there are complications – like indications that the twisted intestine is dying or causing infections, or the intestine has ruptured causing inflammation and infection in the abdomen – immediate surgery is recommended.
Surgical options include removing the affected part of the intestine or surgeries designed to fix the intestine in place to prevent it from twisting again. The latter type of surgery is typically not preferred as it has a higher rate of recurrence. If the intestine has not ruptured, the entire offending part can be removed outright during a procedure known as primary resection. If it has ruptured, a Hartmann procedure – where the damaged part of the intestine is removed and the healthy ends are reconnected or temporarily brought out through an opening in the abdomen until the abdomen has healed – can be performed. In some cases, less invasive surgical options may be considered; this depends on the surgeon’s discretion and experience.
For a cecal volvulus, another type of volvulus which specifically affects the cecum – the beginning of the large intestine – the success rates for endoscopic treatment are usually low (around 20%) and there’s a high probability of repeating condition. In this case, the twisted cecum may be untwisted by doctors and fixed in place, however, usually a portion of it will need to be removed. If the organ has deteriorated to a necrotic or dead state, the affected part would be removed, and an ileostomy or colostomy, where the small or large intestine is redirected out through an opening in the abdomen, would be performed. For patients who are too unwell for general anesthesia, a temporary procedure where a tube is inserted through the skin into the cecum can be done until the patient is fit for a definite surgical operation.
What else can Volvulus be?
When a doctor is trying to diagnose a volvulus, which is a kind of stomach twist, they consider a few other health problems that might be causing the same symptoms. These could be:
- Abdominal hernia
- Appendicitis
- Acute mesenteric ischemia (shortage of blood supply to the intestines)
- Colon cancer
- Constipation
- Colonic polyps (small growths on the lining of the colon)
- Diverticulitis (inflamed or infected pouches in the colon)
- Intestinal perforation (a hole in the wall of the intestines)
- Intestinal pseudo-obstruction (muscle or nerve problems causing symptoms similar to a blockage)
- Intussusception (when one part of the intestine slides into another part)
- Chronic megacolon (a large and improperly functioning colon)
- Toxic megacolon (a very inflamed and large colon due to a disease)
- Mesenteric artery ischemia (poor blood supply due to narrowed or blocked arteries to the intestines)
- Ogilvie syndrome (a disorder with symptoms like a blocked intestine, but no blockage)
- Pseudomembranous colitis (inflammation of the colon caused by an infection)
- Rectal cancer
What to expect with Volvulus
Detecting cecal or sigmoid volvulus, two types of bowel obstruction, early is crucial, as delay can lead to serious complications and even death. Cecal volvulus tends to have a higher mortality rate than sigmoid volvulus. If the volvulus is not treated with surgery, the condition can return in 40-60% of cases.
However, performing surgery on patients in a critical condition can also carry risks, with reported mortality rates of 12-25%. It’s therefore important to balance the benefits and risks when deciding on the best treatment approach.
Possible Complications When Diagnosed with Volvulus
If volvulus, a condition where the intestines twist around themselves, is not treated it can lead to serious problems. These include bowel strangulation, where the blood supply is cut off, gangrene (dead tissue), a hole in the bowel (perforation), and inflammation of the lining of the abdomen (peritonitis). Surgery also carries certain complications like:
- Recurrence of volvulus if a conservative surgery approach is used
- Anastomotic leak, which is leakage from an intestinal connection made during surgery
- Infection around the surgical wound
- Abscess in the pelvic region, which is a pocket of pus
- Sepsis, a severe infection spreading throughout the body
- Fecal fistula, an abnormal connection or tunnel between organs or vessels
- Complications resulting from colostomy or ileostomy, procedures to connect the colon or small intestine to the outside of the body through the abdominal wall.
Recovery from Volvulus
For some patients, particularly those with a perforated inflammation of the peritoneum (the lining of the inner wall of the abdomen), or those who have undergone surgery to remove diseased bowel tissue and reconnect healthy parts, eating and drinking may need to be delayed. In these cases, a tube inserted through the nose into the stomach, known as a nasogastric tube, can allow for ideal decompression of the bowel.
In situations where a large part of the small bowel has to be removed, and the patient needs to fast for a longer time, Total parenteral nutrition (TPN), which provides all the nutrients one needs directly through their veins, can be considered.
Furthermore, patients who have had a colostomy or ileostomy, medical procedures to create an opening in the abdomen for the discharge of body wastes, along with their families, will need to be taught how to take care of these openings.

radiograph.
Preventing Volvulus
It is important for older adults to understand the different factors that can increase the risk of experiencing a twist in the colon, known as a colonic volvulus. These factors can include long-term constipation, a high intake of fiber, consistent use of enemas or laxatives, and connections with mental health disorders or muscle diseases. Neuroleptic drugs, which are used to treat mental health conditions, can also contribute to this condition.
Similarly, Chagas disease or a condition known as megacolon, where the colon is abnormally large, can also make a person more susceptible to a sigmoid volvulus, a specific kind of twist in the lower part of the colon. In rare cases, an inflamed appendix or surgery can lead to excessive scar tissue, which in turn can lead to a volvulus.
It is also crucial for patients to be informed about the various treatments available for a colonic volvulus. These can range from less invasive measures to more extensive surgical procedures. In some cases, surgery might involve the creation of a special opening in the stomach (known as an enterostomy) to allow waste to be removed from the body. This could include a colostomy or an ileostomy.
All potential treatment options and any possible complications should be explained to patients before they undergo surgery for a volvulus, to help them make an informed decision about their care.











