What is Ebstein Anomaly and Malformation?
Ebstein anomaly is a rare heart defect one can be born with, affecting the tricuspid valve and the right lower chamber, or ventricle, of the heart. It accounts for less than 1% of all congenital heart defects. The condition was named after pathologist Wilhelm Ebstein who was the first to describe it in 1866. This anomaly is associated with the following distinct features:
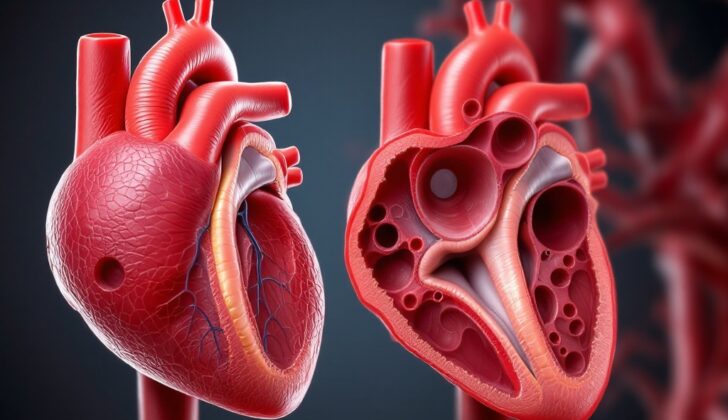
- The tricuspid valve, which controls blood flow between the right upper and lower chambers of the heart, is misplaced towards the tip of the heart.
- Parts of the tricuspid valve are sticking to the heart muscle.
- There’s a stretch and shift in the ring-like structure of the tricuspid valve towards the tip of the heart.
- The part of the right ventricle near the tricuspid valve is enlarged.
- The front part of the tricuspid valve is abnormally formed, often with small holes and attachments.
Typically, patients with Ebstein anomaly may have other heart defects like a hole in the wall separating the two upper chambers of the heart, or an obstruction in the passage of blood from the right ventricle to the lungs. Some newborns may have a blockage in the lungs that affects their breathing. Less common heart defects include holes in the wall separating the two lower chambers of the heart, a combination of four heart defects known as tetralogy of Fallot, an abnormal connection of the major blood vessels of the heart, and defects in the walls separating all four chambers of the heart.
The severity of Ebstein anomaly can vary from having no symptoms at all to severe cases depending on how much the tricuspid valve is shifted and how much it leaks, the size of the right ventricle, and any additional heart defects.
Fast heart rhythms, including conditions like atrial fibrillation, atrial flutter, or out-of-place fast heart rhythms, can occur in 25% to 65% of patients with Ebstein anomaly. Furthermore, 10% to 25% of patients may have extra electrical paths in their heart that can lead to prolonged periods of fast heart rhythms that can potentially result in heart failure and sudden cardiac death.
What Causes Ebstein Anomaly and Malformation?
Ebstein anomaly is believed to be linked with certain changes in chromosome 15q during the development of the heart before birth. Some cases suggest that there might be a link between this condition and changes in chromosome 11q as well. Moreover, it’s been reported that this anomaly could be related to changes in the MYH7 gene, which is commonly connected to heart diseases.
Ebstein anomaly can also be associated with alterations in the NKX2-5 gene. This gene produces a protein that has key functions in heart development and its changes can cause other issues like a hole in the wall (atrial septal defects) between the heart’s upper chambers or issues with the heart’s electrical signals (atrioventricular conduction defects). The NKX2-5 gene is also connected to another heart defect called ‘tetralogy of Fallot’.
The medicine lithium, primarily used as a mood stabilizer, is known to have a negative impact on the development of the fetus, causing conditions like Ebstein anomaly. Studies conducted on pregnant women taking lithium in the 1970s and 1980s indicated that less than 2% of their babies had this heart defect. Additionally, Ebstein anomaly can be associated with a mother’s exposure to certain types of drugs (benzodiazepines) and chemicals found in varnishing materials during pregnancy.
Risk Factors and Frequency for Ebstein Anomaly and Malformation
Ebstein anomaly is a rare congenital heart defect, making up about 0.3% to 0.6% of all birth heart defects. It happens in about 0.2 to 0.7 out of every 10,000 live births. Most of the time, there’s no clear cause for this anomaly. However, some studies suggest it may be inherited in families, especially among identical twins.
- Ebstein anomaly makes up around 0.3% to 0.6% of all birth heart defects.
- It occurs in about 0.2 to 0.7 out of every 10,000 live births.
- Most cases do not have an identifiable cause.
- Some research suggests it might run in families, as seen among identical twins.
- There’s a higher chance (6%) of the condition occurring again in the children of affected women, compared to the children of affected men (1%).
Signs and Symptoms of Ebstein Anomaly and Malformation
Ebstein anomaly is a condition that can manifest differently based on the individual, with some people showing symptoms from infancy or childhood, while others may not present symptoms until adulthood. In some cases, this condition can even be detected in unborn babies. It’s identified through an unusual position of the heart’s tricuspid valve and issues with blood not properly flowing through the heart. Such cases can at times have an enlarged heart. There is a risk of mortality even before and shortly after birth, with instances being higher when the condition is detected before 32 weeks of pregnancy, when certain features of the heart are more pronounced, and with the presence of excess fluid in the heart sac.
Newborns and infants with Ebstein anomaly often have a bluish skin cover, found in about half of the cases. Even so, children showing no such signs have a better chance of surviving to early childhood. As the child grows, signs of heart-related issues may arise. A giant bulge may be noticeable in the neck pulse because of severe backflow of blood from the lower to the upper heart [right ventricle to the right atrium]. If the backflow is too large, this might not be visible. Other noticeable features might include an unusually loud first heartbeat noise due to the front flap of the tricuspid valve shutting, and the splitting of the first heart sound due to a late closure of the tricuspid valve. A constant murmur might also be heard due to the backflow of blood in the tricuspid valve, along with multiple ejection clicks caused by a highly active front leaflet.
On transitioning into adulthood, more than one-half of these patients may experience irregular and frequently fast heartbeats, with such instances being the initial symptoms for about 40% of newly diagnosed cases. In older adults, it’s common to observe symptoms of breathlessness during exercise, resulting from unusual right-to-left blood movement, causing low oxygen levels in the blood. Chronic exhaustion and swelling in the lower extremities could be seen in patients who develop heart failure. Rare and severe complications like stroke, a brain infection, or a heart attack can occur because of abnormal blood clots moving across a heart hole. Normal physical examination in adults usually reveals a murmur due to reflux of the tricuspid valve. Severe cases may indicate over-energetic heart beating and palpable vibrations on the lower left chest area. The second heartbeat sound may be observably distant in case a hole is present in the wall partitioning the upper heart chambers or the right side’s heartbeat-coordinating pathway is blocked.
- Abnormal positioning of the tricuspid valve in unborn babies
- Bluish skin in newborns and infants
- Visible neck pulse fluctuation
- Loud first heart sound and split sound due to tricuspid valve abnormalities
- Murmur due to reverse blood flow
- Frequent fast heartbeats and exertional breathlessness in adults
- Chronic fatigue and lower limb swelling from heart failure
- Potential severe complications like stroke, brain infections, heart attack
- Rumble from the tricuspid valve, vibrations on the lower left of the chest in severe cases
Testing for Ebstein Anomaly and Malformation
In patients with Ebstein anomaly, a heart condition present at birth, changes can typically be seen in their electrocardiogram (ECG), which is a test that measures the electrical activity of the heart. Some of the abnormalities found could include a right bundle branch block (RBBB), which is a delay or blockage along the pathway that sends electrical impulses to the right side of your heart. Delta waves, a type of unusual wave pattern, might appear due to an extra pathway in the heart. Signs of an enlarged right atrium, the top chamber on the right side of the heart, might also be seen in the form of tall P waves.
About 42% of patients with this condition might have first-degree atrioventricular (AV) block, which is slow moving signals from the upper chambers of the heart to the lower chambers. Other irregular heart rhythms can also occur, most commonly atrioventricular reentrant tachycardia, a fast heart beat that starts in the upper chambers of the heart, but also atrial fibrillation, atrial flutter, and atrial tachycardia, which are other irregular heartbeats.
For imaging of the heart and the chest, the first step is often a chest X-ray which can show an enlarged heart particularly on the right side, and might make the heart appear round. An abnormally high cardiothoracic ratio, the ratio of the transverse diameter (width) of the heart to the internal diameter of the chest, could be seen due to the enlargement of the right atrium.
For further visualization of Ebstein anomaly, echocardiography, which is a test that uses sound waves to produce images of your heart, is typically the first choice. This test could show the displacement of certain heart valves, heart chamber dilation, or “flattening” due to volume overload in the right ventricle, which is the lower right chamber of the heart that pumps blood into the lungs. Color Doppler, a technique used to see the flow of blood in the heart, can help detect a condition called tricuspid regurgitation, which happens when the heart’s tricuspid valve doesn’t close tightly.
Assessing the size and the function of the right ventricle can be a challenge, so often a qualitative assessment is used to evaluate it. This assessment is based on the function of the ventricle and the motion of the septum, which is the wall that divides the left and right side of the heart.
Another helpful tool is cardiac magnetic resonance imaging (cMRI) which can offer additional valuable information about the structure of tricuspid leaflets, one of the components of the tricuspid valve in the heart. cMRI is particularly useful in assessing right ventricular function, as it allows for quantification of the RV ejection fraction, a measurement of how well the right ventricle is pumping blood to the lungs.
In some situations, cardiac computed tomography (CT), a type of imaging test, might be used as well to evaluate right ventricular ejection fraction and the anatomy of the tricuspid valve. This technique can be particularly useful before a surgical intervention on the tricuspid valve to have a clearer picture of the coronary anatomy.
Treatment Options for Ebstein Anomaly and Malformation
For infants diagnosed with Ebstein anomaly, which is a rare heart defect present at birth, the treatment primarily focuses on easing symptoms and improving oxygen levels in the blood. For infants manifesting symptoms of heart failure or a bluish discoloration of the skin due to lack of oxygen (cyanosis), nitric oxide can be administered in inhaled form to ease the pressure on the lung’s blood vessels. For cyanotic infants, a drug called prostaglandin E1 (PGE1) can be administered to help maintain a crucial blood pathway in the heart and lower the pressure on lung’s blood vessels.
For newborns showing symptoms of heart failure, a drug called milrinone is often used to reduce the pressure on the lung’s blood vessels. Certain other drugs, such as epinephrine and norepinephrine, are avoided in these situations due to the potentially increased risk of irregular heart rate. Besides, heart failure symptoms can also be managed using diuretics – medicines that help the body get rid of excess fluid – and other heart-friendly medications.
For cases where heart rate becomes too fast and irregular, treatments with drugs like beta blockers and calcium channel blockers can be beneficial. If these are not effective, other special types of drugs or procedures to control heart rhythm may have to be considered.
In terms of surgical treatment, newborns with Ebstein anomaly are usually carefully monitored as the pressure on the lung’s blood vessels decreases. If surgery becomes necessary, a procedure which connects arteries to ensure adequate blood flow to the lungs and rest of the body might be employed. Less frequently, a more detailed surgery might be required based on certain criteria. It has been observed that waiting for surgery until the heart fails or the right side of the heart doesn’t contract as it should, may lead to poorer outcomes.
In older children and adults with Ebstein anomaly, a surgical procedure that involves reshaping and relocating parts of the heart’s tricuspid valve and fixing the hole present in the atrial septum, the wall that separates the two upper chambers of the heart, may be performed. It is often recommended to carry out a surgical procedure to manage irregular heart rhythms during this operation.
In cases where it is not possible to repair the existing heart valve, it may need to be replaced with an artificial one. In patients with severe dysfunction of the right side of the heart, the choice of the artificial valve becomes crucial to avoid other heart issues.
Procedures performed through a catheter might be useful for some patients unsuitable for surgical repair. These may involve closing a detectable hole present in the wall between two upper heart chambers or managing rapid, irregular heart rhythms.
Finally, to prevent a serious heart infection known as endocarditis, it is recommended that patients with unresolved Ebstein anomaly, artificial heart valves, or those who previously suffered from endocarditis take preventive antibiotic before dental procedures. Anticoagulant (blood-thinning) drugs are advised for patients with Ebstein anomaly presenting with irregular heart rhythms or those with symptoms suggesting abnormal blood clot movement within the heart’s chambers.
What else can Ebstein Anomaly and Malformation be?
Some heart conditions that present symptoms resembling Ebstein anomaly, a congenital heart defect, include:
- Transposition of the great arteries
- Tetralogy of Fallot
- Pulmonary atresia
- Hypoplastic left heart syndrome
- Total anomalous pulmonary venous return
An echocardiogram, a type of heart scan, can help properly diagnose Ebstein anomaly.
The condition may also be confused with the following:
- Congenital tricuspid atresia: This can be distinguished from Ebstein anomaly by certain physical traits. For instance, it lacks the abnormal downward shift and moving back of heart valve flaps that is seen in Ebstein anomaly. This condition also does not show dilation or widening of the annular, thickened flaps with rolled edges, and fusion of tendinous fibers in the heart.
- Uhl anomaly: This condition is marked by a birth defect where heart muscle is missing, leading to heart failure. It often occurs with pulmonary atresia, heart aneurysms, and blood clots. This condition does not show the abnormal displacement of the heart valve flap visible in Ebstein anomaly. The main similarity between Uhl anomaly and Ebstein anomaly is an enlarged right atrium and right ventricle in the heart—telling the two apart can be challenging.
- Aberrant tendinous tricuspid valve chords with tethering of the leaflets: An extremely rare heart defect, characterized by abnormal tendinous chords in the tricuspid valve, which reduce valve flap movement. This leads to severe valve leakage due to incomplete closure. It’s a very rare congenital heart defect.
What to expect with Ebstein Anomaly and Malformation
In patients with Ebstein’s anomaly, a rare heart defect present at birth, factors such as the degree of displacement of the tricuspid valve (a valve in the heart), the amount of leaking of the tricuspid valve, and the duration and extent of right ventricle (one of the heart’s chambers) dysfunction can predict the risk of mortality.
Also, Cyanosis (a condition causing a blue or purple coloration of the skin due to low oxygen levels) and fluid accumulation around the heart present a high risk for mortality for unborn babies and newborns. In neonates born with Ebstein anomaly, the co-existence of a leaking pulmonary valve often results in a poor prognosis. This is because of a circular blood flow pattern, where the blood flows from the artery to the right ventricle, then back to the atrium (a cavity of the heart) through a leaky tricuspid valve. This movement of blood could subsequently lead to a decreased cardiac output i.e., the heart’s capacity to pump blood is reduced.
Patients with this anomaly who do not undergo surgery have survival rates of 90% at 1 year, 75% at 10 years, 50% at 15 years, and 40% at 20 years. A sudden death rate of 8.6% due to heart rhythm disorders has been recorded within the first 50 years. In contrast, patients who do undergo surgery have an overall survival rate of 98% at one year, 94% at 4 years, 90% at 10 years, 86% at 15 years, and 76% at 20 years. After one specific procedure called a cone reconstruction, only 2% of patients need to repeat the surgery at 6 years.
The Celermajer index is a score that uses heart ultrasound imagery to predict mortality. It compares the size of different sections of the heart. If the ratio is less than 0.5, the mortality rate is 0%. If the ratio is between 0.5 to 0.99, the mortality rate increases to 10%. If the ratio is 1.0 to 1.49, it’s 40%. For ratios greater than 1.5, the mortality is 100%.
The Simpson Andrews Sharland (SAS) score is another tool used to predict mortality. It takes into account several factors like the Celermajer index, blood flow through the heart and lungs, and heart size, to create a score. In research studies, a score of 5 predicted 100% mortality, and a score of 3 or less predicted 91% survival.
Possible Complications When Diagnosed with Ebstein Anomaly and Malformation
For patients with an untreated Ebstein Anomaly, these are some of the typical complications:
- Heart failure from issues in either right, both, or fast heart beats
- Continuous irregular heart beats
- Unexpected blockages in blood vessels resulting in heart disease or brain damage due to stroke
- Sudden death due to fast irregular heart beats or heart failure.
In these patients, the long-term indicators of death can also consist of:
- Severe leakage of the tricuspid valve
- Heart size 65% or more of the space inside the chest
- Serious limitation in lung growth and function due to an enlarged heart
- Issues with the left heart chamber operation due to enlarged right chamber adjusting the heart’s separating wall
- Difficulty in performing regular physical activities
- Blue discoloration of the skin due to low oxygen
- Early diagnosis age
Also, after surgical treatment for Ebstein Anomaly, these are common short-term complications:
- Obvious irregular heartbeats
- Need for an additional operation due to substantial remaining leakage or narrowing of the tricuspid valve
Long-term complications demanding further operation might include:
- Continued irregular heartbeats due to an enlarged or scared right atrium
- Progressive tricuspid valve issues
Preventing Ebstein Anomaly and Malformation
Ebstein anomaly is a rare heart defect that a person is born with, and it can manifest in different ways. How serious this condition can be ranges quite a bit. Some newborns with this condition sadly don’t live past infancy, while other adults might not even realize they have it until they’re in their 60s or 70s, with the diagnosis coming as a surprise.
Patients with this condition must learn how to recognize the signs that it may be getting worse. Cyanosis, which means their skin turns a bluish color because of a lack of enough oxygen, is one sign. Other symptoms to look out for include those related to heart failure, like fatigue, weakness, and shortness of breath, and signs of arrhythmia, or irregular heart beats. Irregular heartbeats can cause sensations like fluttering in your chest (palpitations), feeling like you might faint (presyncope), or actually fainting (syncope).











