What is Gigantism and Acromegaly?
Acromegaly and gigantism are medical conditions caused by the overproduction of growth hormone. The most common cause is a tumor in the pituitary gland, which produces this hormone. Gigantism happens when too much growth hormone is produced before a child’s long bones have stopped growing, resulting in them being exceptionally tall. Acromegaly, on the other hand, happens when the overproduction occurs after the bones have stopped growing, leading to unusually large hands, feet, and facial features.
The diagnosis for these conditions is confirmed if the individual has high levels of insulin-like growth factor-1 (IGF-1), which is another growth-promoting hormone. Once diagnosed, the first step in treatment is usually to remove the tumor surgically. However, surgery does not always solve the problem, and further medical treatment, like medication that reduces hormone secretion or radiation therapy, is often needed.
What Causes Gigantism and Acromegaly?
In around 95% of cases, conditions called acromegaly and gigantism are caused by an overactive growth hormone (or GH) produced by a non-cancerous tumor in the pituitary gland. However, these conditions can also be due to a tumor in the hypothalamus (a part of the brain) or due to neuroendocrine tumors in the lung or pancreas leading to an overproduction of growth hormone-releasing hormone (GHRH), a hormone which stimulates the production of growth hormone. In rare cases, cancer in the abdomen or blood can also lead to the overproduction of growth hormone, causing acromegaly.
There are also certain genetic conditions linked to overproduction of growth hormone. These include multiple endocrine neoplasia-1 (or MEN-1), which affects multiple glands in the body; neurofibromatosis, which causes tumors on nerve tissue; Carney complex, which results in multiple types of tumors; and McCune-Albright syndrome, which leads to abnormalities in the skin, bones and endocrine tissues.
In addition, there is a hereditary condition called familial idiopathic pituitary adenomas (FIPA). This is caused by changes, or mutations, in a specific gene called aryl hydrocarbon protein-interacting (AIP). This can be linked to familial acromegaly, a form of the condition that runs in families. Notably, about 25% of those with familial acromegaly usually start showing symptoms during their teenage years, resulting in gigantism – a condition where a person grows excessively tall due to too much growth hormone.
Risk Factors and Frequency for Gigantism and Acromegaly
Acromegaly is a medical condition that affects about 78 out of a million people. On a yearly basis, 10 out of a million people are newly diagnosed with this disease. It affects both men and women equally, with an average age of diagnosis at 44 years old. Younger patients are often seen to have a more severe form of the disease. About one-third of people with acromegaly also have high levels of the hormone prolactin in their blood.
Signs and Symptoms of Gigantism and Acromegaly
Acromegaly is a slow-developing condition that can often take about nine years to diagnose. During this time, people might experience dental, heart, or rheumatic problems. This disorder is typically caused by a large pituitary tumor which can press against areas and cause symptoms like vision difficulties, eye movement issues, and headaches. Additionally, it can lead to high levels of prolactin, which in turn can cause symptoms like milky nipple discharge and decreased sex drive.
Other notable characteristics of acromegaly include:
- Increased size of hands and feet due to bone growth and soft tissue swelling. Patients may notice an increase in ring and shoe sizes. While soft tissue swelling can decrease with treatment, bone changes are permanent.
- Experience of excessive sweating and skin tags, which are common in about 98% of Acromegaly cases. These are due to skin cell growth induced by the growth hormone.
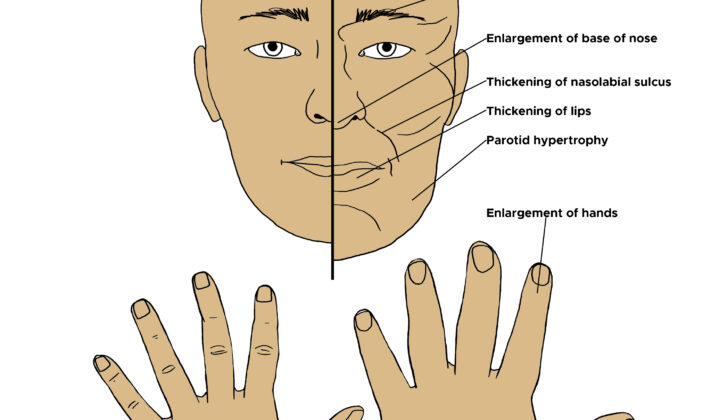
- Changes in the face, which are known as acromegalic facies. This encompasses a wide forehead, broad nose, large lips, acne, prominent chin, enlarged tongue, and coarser facial features. These changes are often subtle and may not be noticed by others. Comparison with older photographs can help identify these gradual changes over time.
- Muscle and bone symptoms, such as generalized weakness, lethargy, misaligned teeth and associated dental complications, and early-onset arthritis due to irregular surfaces in hips, knees, and the spine. A condition called carpal tunnel syndrome, which affects the wrists, may also arise in about 60% of the patients as a result of nerve swelling rather than external pressure.
- Deep or rough voice and obstructive sleep apnea due to swelling of the upper airway and an enlarged tongue.
If a patient is extremely tall, significantly above the average height or more than the adjusted average parental height, they might have gigantism. This rare condition carries associations with certain syndromes such as neurofibromatosis, Carney complex, and McCune Albright syndrome. Hence, examination for neurofibromas with cafe au lait spots, optic gliomas, and skin lentigines should be undertaken.
Testing for Gigantism and Acromegaly
If your doctor suspects you have acromegaly, a condition that is often caused by a benign tumor in your pituitary gland, they will likely start by testing your levels of a substance called IGF-1. IGF-1, which stands for insulin-like growth factor-1, is a stable molecule that usually remains in your body for about 15 hours. People with acromegaly tend to have higher levels of IGF-1, so if your IGF-1 level is normal, you probably don’t have acromegaly. However, keep in mind that some factors can affect IGF-1 levels – for instance, if you’re pregnant, a teenager, or on estrogen therapy, your IGF-1 levels might be falsely high or low. Other conditions such as liver or kidney failure, underactive thyroid, malnutrition, infections, and poorly controlled diabetes could also influence IGF-1 levels.
If your IGF-1 levels are high, your doctor might ask you to do an oral glucose tolerance test (OGTT). This test involves drinking a sugar solution and then testing your blood to see how your body processed the sugar. The doctor will particularly be interested in measuring levels of growth hormone (GH), as a GH level of 1 mcg/lt or less, two hours after drinking the sugar solution, would rule out acromegaly. Before and after the OGTT, your blood glucose levels will be checked to ensure that your body is processing sugar correctly.
Your doctor could also use magnetic resonance imaging (MRI) to get a detailed image of your pituitary gland. MRI can help them see the size and location of any tumors, check whether there’s damage to nearby brain structures, like the optic chiasm which is involved in your vision, and even see if the tumor has spread to your sinuses. If the MRI scan shows that the tumor might be pressing on your optic chiasm, you might need to do a visual field test to check how well you can see in all directions without moving your eyes.
Depending on your symptoms, your doctor might also wish to check your prolactin levels. High levels of prolactin, which is another hormone made in the pituitary gland, can lead to symptoms like galactorrhea (where a milky discharge comes out of nipples) or hypogonadism (where reproductive organs don’t work as they should). You might also need further tests to check how well the rest of your pituitary gland is working.
In very rare cases, where everything with the pituitary appears normal but the biochemical tests are suggestive of acromegaly, your doctor might need to look for the source of the excessive hormones. They could do this by measuring your levels of a hormone called GHRH and doing more imaging tests of your chest and abdomen.
Treatment Options for Gigantism and Acromegaly
The goal of treating acromegaly, a hormonal disorder that results from an overproduction of growth hormone, is fourfold:
1. To remove the tumor in the pituitary gland causing the condition.
2. To bring levels of IGF-1, a hormone that stimulates growth, back to normal.
3. To alleviate the symptoms of acromegaly, which can include enlarged hands and feet, thickened skin, and joint pain.
4. To monitor for the disease and any related health conditions.
To achieve these objectives, doctors may use any combination of three primary treatment methods: surgery, medication, and radiation therapy. The chosen treatment plan will depend on the patient’s individual circumstances.
Surgery is often the first choice for treating acromegaly, unless the patient is not a good candidate for surgical procedures. The preferred method of surgical removal of the tumor is through a minimally invasive approach known as transsphenoidal surgery. In this procedure, the surgeon accesses the pituitary gland through the sphenoid sinus (a hollow space within the bones of the skull) to remove the tumor. Twelve weeks after surgery, the levels of IGF-1 and growth hormone will be tested to see if they have normalized.
If the disease persists after surgery, medication may be used. Dopamine agonists and somatostatin receptor ligands are both types of drugs that can help decrease the secretion of growth hormone. Side effects can include dizziness, nausea, and low blood pressure. Growth hormone receptor antagonists, another type of medication, block the action of growth hormone, thus decreasing its effects. A potential downside is that these medications can be expensive, so they are typically used for patients who don’t respond well to other treatments.
Radiation therapy may also be used after surgery if the disease is still present or as a first line of treatment for patients who can’t undergo surgery. There are two main types: external irradiation and stereotactic single high dose irradiation. External irradiation targets the pituitary gland with radiation, while the stereotactic method delivers a high dose of radiation to a specific, mapped area. A potential side effect of radiation therapy is hypopituitarism, a condition in which the pituitary gland does not produce enough of certain hormones.
The best treatment approach for acromegaly varies from person to person, depending on their overall health, the size and location of the tumor, and how far the disease has progressed. Therefore, it’s crucial for individuals diagnosed with acromegaly to have a detailed discussion with their healthcare team to choose the most suitable treatment plan.
What else can Gigantism and Acromegaly be?
“Acromegaloidism” is a condition where individuals have faces that resemble those with acromegaly (a disorder that results in abnormal growth) or are exceptionally tall. However, this isn’t caused by the same hormonal imbalances found in acromegaly. Medical tests show that levels of growth hormone (GH) and insulin-like growth factor 1 (IGF-1) are normal, and scans of the pituitary gland (which normally triggers increased growth) don’t show any abnormalities.
Another condition, called “Soto’s syndrome”, also has similarities with acromegaly. People with this congenital syndrome are usually tall and have facial features similar to those with acromegaly. They might also have intellectual disabilities, oversized heads, and their bones may age faster than normal. Additional physical symptoms can include weak muscles at birth, heart defects, crossed-eyes, curved spine, and a higher chance of developing cancer. This syndrome is caused by deficiencies in a specific gene on the 5th chromosome, known as the NSD1 gene. Like acromegaloidism, people with Soto’s syndrome have normal levels of GH and IGF-1 hormones. To differentiate it from acromegaly, genetic studies are usually required.
What to expect with Gigantism and Acromegaly
The outlook for a patient largely depends on how early the condition is diagnosed and how well the hormone levels respond to treatment. These treatments could either be surgical (involving a medical procedure) or non-surgical (like medications).
Possible Complications When Diagnosed with Gigantism and Acromegaly
In patients who have acromegaly (an overproduction of growth hormone), there are common complications that can affect a variety of bodily systems, among these are cardiovascular problems, sleep issues, joint troubles, gastrointestinal concerns, cancer risks, hormone imbalances, and bone issues.
Cardiovascular Problems:
- High blood pressure is seen in about 40% of acromegaly patients. It’s usually mild and is treated similarly as in patients without acromegaly. It’s crucial to keep blood pressure under control no matter what treatment is being used for acromegaly.
- Cardiomyopathy (heart muscle disease) is seen in most acromegaly patients. Regular heart exams such as an echocardiogram and ECG should be done. The condition often improves with the treatment of acromegaly, but this improvement can depend on patients’ age, disease duration, and presence of high blood pressure.
Sleep issues:
- About 70% of acromegaly patients experience sleep apnea. Certain conditions that come with acromegaly, like an enlarged tongue, may heighten the risk of sleep apnea. Sleep quality evaluations and if needed, sleep studies, should be done regularly. Surgery can sometimes fix certain conditions that contribute to sleep apnea.
Joint Issues:
- About 75% of acromegaly patients experience joint problems. This can affect any joint and can lead to nerve trapping due to the growth of bone and soft tissue. Diagnosing and treating acromegaly early can prevent these joint issues from happening.
Gastrointestinal concerns and Cancer Risks:
- People with acromegaly often have an increased length of colon and larger mucosal folds. This condition increases the chance of getting colon polyps. It’s unclear if the risk of colon cancer is increased due to acromegaly. Regular colonoscopies should be performed.
- There has been an increase in both benign and malignant tumors in acromegaly patients, including kidney and ureteral cancers. However, this hasn’t tended to increase cancer-based deaths.
Hormone Imbalances:
- Patients with acromegaly can sometimes have a deficiency in pituitary hormones as a result of their treatment (surgery or radiation). Checking the level of pituitary hormones yearly and supplementing when necessary is often recommended.
Bone problems:
- Patients with acromegaly have a higher occurrence of vertebral fractures. Also, a decrease in sex hormones has been linked to bone loss.
Preventing Gigantism and Acromegaly
Patients need to understand the critical role of early detection and the necessity to stick to their treatment plans. Regular checks of the endocrine system, which is the group of glands that produce hormones, are helpful. It’s also important for them to regularly monitor their blood pressure and blood sugar levels.











