What is Avascular Necrosis?
Osteonecrosis is a bone disease in which parts of the bone die because the blood cannot reach them. This condition is also known as avascular necrosis, aseptic necrosis, or ischemic bone necrosis. It usually affects the ends of long bones in joints that carry weight. In severe cases, the disease can damage the bone under the cartilage layer or even cause an entire joint to collapse.
The condition most frequently occurs in the hip, knee, ankle, and shoulder. However, the hip is affected more often than other areas. Osteonecrosis can also occur in other less common parts of the body, such as the wrist and jaw. As a result, recognizing and treating osteonecrosis early is very important.
This topic discusses the causes and development of osteonecrosis, including its symptoms and treatment options for the most common types.
What Causes Avascular Necrosis?
Osteonecrosis, a condition where bone tissue dies due to a lack of blood, is often associated with a decrease in the supply of blood to the subchondral bone (the layer of bone just under the cartilage). However, there are many theories about what could cause this to occur, and there are multiple factors that could increase your risk. These can fall into several categories:
- Direct damage to cells caused by chemotherapy, radiotherapy, heat injury, or smoking.
- Arterial fractures outside the bone (which can be caused by things like hip dislocation, femoral neck (top of thigh bone) fractures, issues caused by surgery, or born with abnormal arteries).
- Issues with the veins outside the bone that could cause a slower blood flow.
- Anything that compresses the veins inside the bone, like excessive bleeding, high bone marrow pressure, cell enlargement and marrow infiltration, bone marrow swelling, and displaced fractures.
- Bone marrow becoming fatty because of long-term use of high-dose corticosteroids.
- Blood clotting issues and obstructions in blood vessels inside the bone, such as coagulation disorders, sickle cell crises, or other factors that are not yet well-understood.
In some cases, genetics may play a role, for example, certain mutations in the COL2A1 gene that directs the production of type 2 collagen have been tied to osteonecrosis. However, in many cases, no clear cause can be found; this is referred to as idiopathic osteonecrosis.
Moreover, physical activities involving repetitive strain, such as assembly line work, can pose a risk. Non-traumatic risks can include any factor that might affect the bone’s blood flow. Radiation can cause changes in bone marrow and lead to osteonecrosis. High cholesterol can block small blood vessels, cutting off the bone’s nutrient supply. Conditions like sickle cell anemia can compromise the bone’s blood supply.
Bones with anatomical peculiarities, like a low ability for blood flow rerouting or backward blood flow, are at a higher risk of necrosis. Moreover, unique anatomy like that of the talus which is largely covered by joint cartilage makes the area less receptive to blood flow.
Prolonged, high-dose use of glucocorticoids can also result in osteonecrosis by destroying individual bone cells, disrupting the system of small canals for nutrient/waste exchange. Other risks include alcohol misuse, blood disorders, autoimmune diseases like lupus, etc. For 25% of people with osteonecrosis, the cause remains unknown. For instance, in Kienböck and Preiser disease, the exact cause of osteonecrosis usually can’t be pinpointed.
Risk Factors and Frequency for Avascular Necrosis
Osteonecrosis often occurs in larger bones like the hip, humerus, knee and talus, but it’s less common in smaller bones like those in the wrist. While it can affect the jaw, we’re focusing here on the types of osteonecrosis typically treated by an orthopedic surgeon.
- About 10% of hip replacements in the U.S. are due to osteonecrosis, mostly seen among people 30 to 65 years old.
- Osteonecrosis affects men more frequently overall, but autoimmune conditions like lupus, which women are more likely to have, also play a significant role.
- Less common variations like Preiser disease, osteonecrosis of a wrist bone called the scaphoid, are usually found in the dominant hand of middle-aged men.
- Another variant, Kienböck disease, (osteonecrosis of another wrist bone, the lunate), is often seen in middle-aged men who do manual labor. It has also been reported in children.
Signs and Symptoms of Avascular Necrosis
Osteonecrosis is a condition that can affect various areas of the body, including the hip, knee, shoulder, talus (ankle), and the lunate and scaphoid bones in the wrist. This condition typically causes pain, and the severity of symptoms often varies depending on the stage of the disease and the specific body part involved. Here’s a breakdown of the common symptoms associated with osteonecrosis based on anatomical location:
- Hip: No symptoms in early stages. Later, sufferers might experience hip and groin pain, stiffness, changes in walking style, and referred pain in the buttock and thigh.
- Knee: Acute pain in the knee when weight-bearing and at night, tenderness over the medial part of the knee and decreased range of motion.
- Shoulder: Pulsating pain that can extend to the elbow and a decrease in active range of motion usually associated with osteonecrosis in other body parts or trauma.
- Talus (Ankle): Pain and difficulty walking, especially beyond the expected recovery time after a traumatic event.
- Lunate and Scaphoid (Wrist): Pain on the back and outer side of the wrist, decreased range of motion, wrist swelling, and weakened grip strength. This’s usually common among skilled laborers and can occur without prior trauma to the wrist.
It’s important to note that the onset and intensity of these symptoms can vary widely from case to case. Additionally, certain factors such as recent trauma, steroid use, autoimmune disease, sickle cell disease, alcoholism, tobacco use, changes in walk style, and connective tissue disorders can potentially contribute to the onset and progression of osteonecrosis.
Testing for Avascular Necrosis
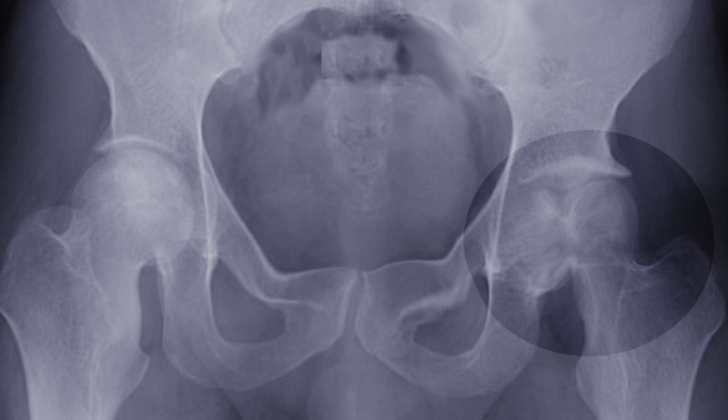
The early detection of a disease affecting the bones often starts with plain radiographic films from two different angles. Though in the beginning stages of the disease, these pictures may look normal. For finding out the disease in its earlier stages, Magnetic Resonance Imaging (MRI) is recommended as it is very effective at detecting bone edema, which is when excess fluid gets trapped in the body’s tissues.
Osteonecrosis is a disease that primarily affects the hip, knee, shoulder, talus (a bone in the ankle), lunate (a bone in the wrist), and scaphoid (a small bone on the thumb side of the wrist). This disease in your hip could be because of injury or not, with the non-injury related cases possibly affecting both hips. Familiar systems to classify these disease phases are Ficat or Arlet and Steinberg classifications. Ficat and Arlet describe the four stages of disease progression, starting from the disease’s initiation without any signs in radiological findings to the end stage featuring the collapse, flattening, and narrowing of the joint space in your hip.
Spontaneous osteonecrosis of the knee (SONK) is the most common type affecting the knee, with a secondary type that is common in young people and often linked with several risk factors. A rare type is post-arthroscopic osteonecrosis, seen in about 4% of patients after an arthroscopic meniscectomy – a small surgery to repair the meniscus in the knee. SONK most commonly presents in those who are in the sixth decade of life and tends to affect more females than males.
Osteonecrosis of the shoulder most often results from injury, although it can be caused by issues highlighted above, such as long-term high-dose corticosteroid use. Hertel et al. found connections between certain fracture and reduced blood flow to the head and also found factors such as the length of the posteromedial metaphyseal head extension and the integrity of the medial hinge were critical for osteonecrosis’ occurrence.
Osteonecrosis of the talus, which is most commonly caused by injury, results in fractured bones in the neck of the talus. Avascular necrosis becomes more likely with a concurrent dislocation at the ankle or subtalar joint – the joint just below the ankle. The disease is best described by the Hawkins classification.
Osteonecrosis of the lunate, more commonly known as Keinbock disease, involves a collapse of the lunate due to inadequate blood supply and osteonecrosis. Reasons for this disease may include a history of repetitive injury, biomechanical factors related to ulna variance (a condition where the ulna, one of the bones in the forearm, is longer or shorter than the other), and anatomic factors.
Osteonecrosis of the scaphoid, known as Preiser disease, arises from an unclear cause. Risk factors include alcohol abuse, trauma, steroid use, and connective tissue disorders. Generally, it affects the dominant hand of those in their middle age, although it can occur on either hand. The Herbert and Lanzetta classification system is used to track disease progression.
Treatment Options for Avascular Necrosis
Treatment for a condition known as osteonecrosis, which involves bone tissue death, is varied and can range from noninvasive methods to surgery depending on the severity of the disease and which joint is affected.
When focusing on the hip, using medicines such as Alendronate only or in combination with bisphosphonates is a debated method. These drugs can be helpful in early-stage disease by slowing its progression and preventing bone collapse, but they may take some time to relieve pain. On the other hand, many patients may eventually need a total hip replacement. However, a procedure called core decompression could be a good alternative in the early stages of the disease, especially if it’s affecting just a small portion of the weight-bearing part of the hip bone. This process safely reduces pressure inside the bone and stimulates healing, particularly if used along with a bone graft.
If the disease is in a position where it can be moved away from the weight-bearing surface, a procedure called rotational osteotomy might be beneficial. However, this can make future hip replacement surgeries more difficult. For patients who are older or with larger or more advanced lesions, a total hip replacement could be the best option, often providing good results for reducing pain and improving function. However, for younger patients doing heavy work, fusing the hip joint could be considered.
In terms of the knee, many cases of spontaneous osteonecrosis can be resolved with weight-bearing limitations and exercises to strengthen the quadriceps muscle. For more severe cases, knee replacement surgery, either partial or total, might be needed.
Regarding the shoulder, non-surgical treatment involving pain management, physiotherapy, and activity modification is usually the first step. If the disease progresses, surgical options include core decompression for mild disease, and placement of a resurfacing implant or half-joint replacement for moderate disease. For advanced disease stage, a total shoulder replacement may be undertaken.
In the case of the ankle, reducing the risk of osteonecrosis often involves surgical repair of any ankle bone fractures.
For issues with the lunate bone in the wrist (Keinböck Disease), early treatment focuses on trying to restore blood supply to the affected bone or taking pressure off it. Surgery might be necessary if the disease is advanced. Similarly, in Preiser Disease, which specifically affects the scaphoid bone in the wrist, treatment often inevitably involves surgery as the disease progresses.
What else can Avascular Necrosis be?
The conditions that doctors need to consider when diagnosing a patient might include:
- Bone marrow edema syndrome (also known as transient osteopenia) – a temporary bone condition
- Complex regional pain syndrome – a chronic pain condition
- Inflammatory synovitis – inflammation of the synovial membrane in joints
- Neoplastic bone conditions – conditions where abnormal growths occur in the bone
- Osteoarthritis – a degenerative joint disease
- Osteochondrosis – a family of orthopedic diseases in adolescents
- Osteomyelitis – inflammation of bone caused by infection
- Osteoporosis – a disease that weakens bones and makes them brittle
- Rheumatoid arthritis – a chronic inflammatory disorder affecting the joints
- Septic arthritis – a painful infection in a joint
- Soft tissue trauma like labral tears or meniscal tears – injuries to the cartilage in the hip or knee
- Subchondral fractures – a break or crack just below the cartilage of a joint
By considering these different possibilities, doctors can make a more accurate diagnosis.
What to expect with Avascular Necrosis
Osteonecrosis often has a poor outlook, regardless of initial treatment. The disease can lead to ongoing pain, disability, and deterioration beyond the point of repair. A study showed that 59% of initially symptomless cases eventually developed symptoms or collapsed. In particular, AVN of the humeral head, or the shoulder joint, can be more critical. As many as 81% of patients progressed to total failure, which required an arthroplasty, or a joint replacement.
A couple of methods, namely core decompression and bone grafting, can prevent the worsening of hip osteonecrosis. However, if the disease has advanced or joint-saving treatments fail, a total hip replacement becomes necessary but can lead to a higher risk of complications.
For early stages of AVN in the shoulder, core decompression and hemiarthroplasty have shown positive results. But, total shoulder replacements, while an option for severe AVN cases, has a higher chance of post-surgery complications.
In the case of Preiser and Kienböck diseases, early stages of AVN can be treated with immobilization. However, it usually leads to the need for surgical intervention. Surgical repair of the talus (ankle bone) in AVN management tends to yield better results in younger patients.
Possible Complications When Diagnosed with Avascular Necrosis
After an operation for osteonecrosis, several complications may arise. These include infections at the site of the surgery, prosthesis breaking down, and damages to the nerves and blood vessels. The disease often continues to progress even after surgery, leading to high failure rates. For instance, in 90% of cases, the disease in the hip joint continued to progress even after a core decompression surgery. In Kienböck disease, if the patient’s unique anatomy is not considered during an osteotomy of the radius, it can result in excessive ulnar variance (a condition where the ulna is longer than the radius) and pain in the ulna after surgery.
Existing health conditions of the patient can also greatly affect the rate of complications. For example, in patients with sickle cell disease who had undergone a total joint replacement for osteonecrosis, there were longer hospital stays, higher chances of acute kidney injury, implant failure, pulmonary embolism, deep vein thrombosis, heart attacks, and a considerably higher death rate.
Rephrased potential complications:
- Infections at the site of the surgery
- Breakdown of the prosthesis
- Damage to the nerves and blood vessels
- Persistent progression of the disease despite having the surgery
- Excessive ulnar variance and pain in case of Kienböck disease
- Longer hospital stays
- Increased chances of acute kidney injury
- Chances of failure of the implanted joint replacement
- Increased risk of pulmonary embolism
- Increased chances of deep vein thrombosis
- Risk of heart attacks
- Higher death rates
Preventing Avascular Necrosis
Osteonecrosis often begins before any obvious symptoms show up. If not treated, it often advances to its final stage, causing extreme pain, difficulty with movement, and even the collapse of joints. The way this disease affects people can vary greatly.
To lessen the likelihood of experiencing osteonecrosis, it’s important to maintain a healthy lifestyle. This means moderating alcohol intake, avoiding tobacco, and only using corticosteroid medications as necessary, under instruction from your doctor. Other beneficial habits include eating healthily and keeping a suitable weight, which can help prevent damage to your joints.
For people whose jobs involve physical labor, taking steps to avoid repetitive tasks that strain the joints is key. If possible, it is also recommended to take regular breaks. Lastly, it’s important to regularly check in with your healthcare provider, even if you feel fine. This is because osteonecrosis can often start developing without causing any notable symptoms. Regular check-ups can catch any issues early and stop them from becoming more serious.











