What is Stener Lesion?
Ulnar collateral injuries of the thumb are quite common and can vary in severity. These injuries can stretch from a mild sprain to a partial or full tear in the ligament. Sometimes, small fragmented bones can also be torn off from the base of the thumb.
Full thickness ruptures, where the ligament is completely torn, can either be non-displaced (where the ligament stays in place) or displaced (where it moves from its normal position).
Understanding whether the tear is displaced or not is important. When a certain ligament known as the UCL is displaced, it may get caught in a nearby muscle, the aponeurosis of the adductor pollicis, and this can have treatment implications. This theory was first described in 1962 by Bertil Stener, a Swedish surgeon. Thus, it’s named the Stener lesion after him.
The role of the UCL in the thumb is to provide stability and balance to the thumb during a forceful grip. This ligament comprises of two parts: the proper collateral ligament and the accessory collateral ligament.
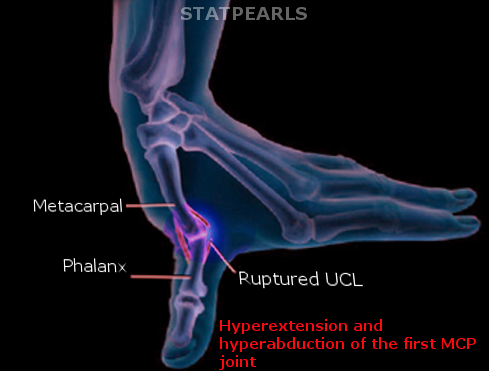
A Stener lesion happens when the thumb undergoes a forceful outward twist. This leads to the tearing of UCL from its point of attachment at the base of the thumb. The torn end can get trapped in the adductor aponeurosis muscle and isn’t able to return to its usual position. This results in an unstable thumb, and is a common injury seen in people such as skiers and gamekeepers.
What Causes Stener Lesion?
The UCL, or Ulnar Collateral Ligament, is a band of tissue that connects the bones in the thumb. It can be injured if the thumb is forced into extreme positions, like being pulled strongly back and to the side. This sort of injury was first noted among Scottish gamekeepers who would kill rabbits in a manner that put a lot of strain on their thumbs. After many times of doing this, their thumbs would become unstable and weak. This injury is often called “gamekeepers thumb”.
Interestingly, similar injuries can occur in modern times from falling on an outstretched hand while holding something like a ski pole. This is sometimes called “skier’s thumb”. Even though “gamekeepers thumb” and “skiers thumb” are used interchangeably, the first term generally refers to a long-term UCL injury while the second term refers to a sudden, extreme bending of the UCL.
Additionally, sports like hockey, soccer, handball, basketball, and volleyball can cause this same type of injury. Interestingly, there was a case where someone injured their hand this way while doing a handstand.
Sometimes, if the UCL is torn, it can get trapped over the tissue connecting the muscles in the thumb, creating what’s called a “Stener lesion”. This scenario was initially described by a doctor named Stener.
Risk Factors and Frequency for Stener Lesion
Every year, around 200,000 people injure the ulnar collateral ligament (UCL) in their thumbs. Stener lesions, a specific type of these injuries, happen in 64% to 87% of all complete UCL ruptures. Thumb injuries are especially common in skiing, making up to 32% of all skiing-related injuries. However, UCL ruptures are rarely seen in children.
- About 200,000 UCL thumb injuries occur every year.
- 64% to 87% of all complete UCL ruptures involve Stener lesions.
- Up to 32% of all ski injuries are thumb injuries.
- UCL ruptures are not common in children.
Signs and Symptoms of Stener Lesion
Individuals with injuries to the UCL, a ligament in the thumb, might notice things like swelling, bruising, and tenderness on the side of the thumb closest to their body. They could also find that their thumb feels unstable and that they have trouble with actions that require a strong grip or pinching something between thumb and finger. In some cases, a lump could be felt near the joint of the thumb, which could indicate a type of injury known as a Stener lesion. However, this isn’t a definite sign of such an injury.
Examinations that put stress on the thumb joint don’t clearly separate minor UCL injuries from major ones, even when the joint appears unstable. Furthermore, doctors need to be careful not to exacerbate the injury during these tests, as they could potentially worsen a slight tear into a major one. There are also other conditions that can trigger thumb joint pain, which makes UCL injuries tricky to diagnose without using medical imaging.
In medical images, acute UCL injuries can be classified in the following ways:
- Type 1: A non-displaced tear.
- Type 2: A fracture in the thumb’s base.
- Type 3: Strain on the ligament.
- Type 4: A full tear of the UCL.
- Type 5: No injury to the UCL, with a detached plate on the under surface of the thumb.
Testing for Stener Lesion
Plain film X-ray is often the first step in looking at injuries to the hand, including fractures and issues with the MCP joints, which connect each finger and the thumb to the hand. If there’s a broken piece of bone in the proximal phalanx (the bone in your finger nearest to your hand), it might suggest a UCL injury. If this bone is moved more than 1 millimeter from where it should be, this can indicate a more serious UCL tear.
However, the X-ray might look normal even if you have a gamekeeper’s thumb injury. As a result, if your doctor is reasonably certain that you have this injury or if they suspect a “Stener lesion” (where the UCL has been dislocated), they may order further tests.
Arthrography, a type of imaging that uses a contrast agent with magnetic resonance or MR imaging, is known to be reliable when checking for UCL injuries. While it does have a high level of accuracy, MR imaging can be costly and may not be readily available.
Ultrasound imaging has been gaining attention in medicine because it is not invasive, more affordable, and quicker. According to studies, ultrasound can accurately identify between a UCL tear that has stayed where it should be and one that has moved out of place. Experienced technicians can use ultrasound to diagnose a Stener lesion with a high level of accuracy.
Ultrasound is dynamic, meaning it can create real-time images. This allows for the easy viewing of how the UCL relates to the adductor aponeurosis, a broad, flat tendon which acts as the insertion point for muscles. When the joint where the thumb joins the hand is bent and the ultrasound is done, it can make a distinction between a UCL tear that hasn’t moved and a Stener lesion. Also, it gives a quick insight into the healthy side to compare.
A Stener lesion seen on an ultrasound has been described as resembling a “tadpole sign” or a “yo-yo on a string sign”. To explain, the “head of the tadpole” is made of the part of the UCL (which has retracted, or pulled back) next to the base of the finger or thumb bone. The “tail” of the tadpole is made of the adductor aponeurosis, which often appears thicker and is located beneath the pulled-back UCL fibers. The “yo-yo on a string” is formed when the small lump, caused by fibers from the torn ligament which has pulled back, sits next to the adductor pollicis muscle. The “yo-yo on a string” sign can also be seen on an MRI.
Treatment Options for Stener Lesion
When treating a gamekeeper’s thumb, which is an injury to the ulnar collateral ligament (UCL) in your thumb, the main aims are to ease and eventually ease the pain, prevent instability of the thumb joint, and to try and prevent a type of joint disease called osteoarthritis. Not every UCL injury requires surgery. Often, a splint that immobilizes the thumb and sometimes part of the arm is used. Usually, this splint is needed for a few weeks.
However, surgery is needed if a certain type of injury, called a Stener lesion, is present. This is because the Stener lesion makes the ligament tears separate too much, preventing the healing process. In this case, the surgeon will use a “bone anchor” to re-secure the torn ligament.
The specific treatment depends on the severity and type of the UCL injury:
- Type 1 injuries, where the UCL tear is very small or not really displaced (moved), can often be healed with just immobilization using a splint.
- Type 2 injuries are slightly more severe, with the UCL being displaced by less than 3 millimeters. However, these can also generally be healed with immobilization.
- Type 3 injuries are more severe, with UCL tears displaced by more than 3 millimeters. Usually, immobilization will not be enough to heal these injuries, and surgery will be necessary.
- Type 4 injuries are Stener lesions. These will always require surgery.
A splint is still the first option for type 1, 2 and some type 3 injuries – the thumb will be immobilized in what’s called a thumb spica for around 4 weeks.
Chronic UCL injuries, which have persisted for a long time, can be difficult to repair. If the patient has moderate to severe arthritis, then a medical procedure known as arthrodesis can be done on the main thumb joint. If there’s no arthritis, then the ligament can be reconstructed or the tendon advanced. These are both surgical options.
What else can Stener Lesion be?
There are a number of conditions that can appear similar to a UCL injury, including:
- Tear in the Dorsal hood
- Thenar Muscle Injury
- Injuries to the Radial collateral ligament
- De Quervain disease
- First carpometacarpal joint osteoarthrosis
- Vascular injury to the superficial branch of the radial artery
- Volar plate injury
- Tear in the Extensor pollicis longus
- Trigger thumb
- Tendinosis in the Flexor carpi radialis tendon
- Rupture in the Flexor pollicis longus tendon
What to expect with Stener Lesion
In cases where the UCL, or Ulnar Collateral Ligament (a ligament in the elbow), is completely ruptured, 90% of patients show good-to-excellent outcomes if it is treated within 3 weeks, no matter the type of repair method used.
However, if treatment or diagnosis is delayed, it often leads to larger, more complicated surgeries, and usually, the overall outcome tends not to be as good.
Possible Complications When Diagnosed with Stener Lesion
If UCL (a ligament in the thumb) injuries are not diagnosed or treated promptly, it can affect the recovery process and delay the return to normal activities. Ignoring or missing out on a diagnosis of Stener lesions (where the ligament is displaced) can cause long-term thumb pain, instability, and osteoarthritis (a type of joint disease). Surgery is required to fix a Stener lesion, but there could be complications from the procedure. Some reported complications include temporary numbness due to damage to the radial nerve (a nerve in the arm), repeated instability and stiffness in the thumb joints.
Main Points:
- Quick diagnosis and treatment of UCL injuries is essential for a good recovery
- Untreated Stener lesions can lead to chronic thumb pain, instability, and osteoarthritis
- Surgery is necessary to fix a Stener lesion
- Possible side effects of surgery include sensory damage to the radial nerve, recurring instability, and thumb joint stiffness
Recovery from Stener Lesion
After surgery, it’s standard practice to immobilize the surgical area for six weeks as a part of the recovery process. About three months after the operation, patients can typically resume their regular activities without any restrictions. However, some medical professionals recommend wearing a thumb support (called a “thumb spica”) for about 1 to 4 weeks after the operation. This is followed by doing exercises which involve bending and straightening the thumb, also known as flexion-extension exercises, to regain mobility and strength.
Preventing Stener Lesion
Injuries to the UCL (Ulnar Collateral Ligament, a ligament in the elbow), can sometimes be overlooked by healthcare professionals who might not be experienced in identifying this specific type of injury. Furthermore, patients might also delay getting medical help, especially if the injury happened while they were on vacation (for instance, while skiing). Similarly, they might wait to get medical attention if their initial X-rays didn’t show any abnormality, or they might decide to visit their usual doctor once they’re back home.











