What is Tolosa-Hunt Syndrome?
Tolosa Hunt Syndrome (THS) refers to a condition where you have a severe headache around one eye coupled with eye pain and difficulty in moving the eye. Other names for Tolosa Hunt Syndrome include painful ophthalmoplegia (eye muscle weakness), recurrent ophthalmoplegia (repeated cases of eye muscle weakness), or just ophthalmoplegia syndrome. This syndrome is recognized as one of the rare disorders by the National Organization for Rare Disorders (NORD), a group dedicated to helping people with rare diseases.
It’s also categorized under painful cranial neuropathies (conditions involving nerve damage in the head) by the International Headache Society (IHS), which is responsible for classifying different types of headaches. The first ever description of this syndrome was given by a Spanish neurosurgeon, Dr. Eduardo Tolosa, in 1954. Other similar cases were reported in 1961, and then it became widely known as Tolosa Hunt Syndrome in 1966, named after the early researchers. Before this, it wasn’t a well-recognized condition. Since then, the syndrome has been studied around the world numerous times.
What Causes Tolosa-Hunt Syndrome?
Tolosa Hunt syndrome is typically unexplained and believed to be caused by a general inflammation around the areas of the cavernous sinus (a large vein at the base of the brain) and/or superior orbital fissure (a gap in the bones around the eye). However, it could be triggered by a physical injury, growths, or an aneurysm (a bulging blood vessel).
Risk Factors and Frequency for Tolosa-Hunt Syndrome
Tolosa Hunt syndrome is a rare condition, with approximately one case per million people worldwide each year. This syndrome doesn’t favor any specific geographical location or racial group. It’s relatively uncommon in young people, with the average age of onset around 41 years old. While it typically affects one side of the body, there have been cases where both sides are affected, although these are relatively few (about 5% of cases). It’s also equal opportunity – it affects males and females alike.
Signs and Symptoms of Tolosa-Hunt Syndrome
Tolosa Hunt syndrome is a condition associated with a very intense pain that usually affects the areas around or behind the eye, and may spread to the forehead and the sides of the head. This pain typically appears first, often up to a month before other symptoms such as ophthalmoplegia, which is the paralysis or weakness of eye muscles. This condition’s pattern typically involves it flaring up and then subsiding for periods of several months or even years.
Accompanying symptoms often involve several nerves associated with eye movement and general facial senses. The most commonly affected are the:
- Oculomotor nerve (about 80% of cases)
- Abducens nerve (around 70% of cases)
- Ophthalmic branch of the trigeminal nerve (approximately 30% of cases)
- Trochlear nerve (roughly 29% of cases)
In roughly 20% of cases, the third-order neuron Horner syndrome might occur, which affects the pupil of the eye. Other less common symptoms can include involvement of nerves controlling overall facial sensation and movements, and even the optic nerve, which can potentially lead to vision issues.
Remarkably, Tolosa Hunt syndrome usually doesn’t involve other neurological or systemic symptoms. However, intense pain can cause nausea and vomiting, which usually get better once the pain is under control. Fatigue has been reported too. Symptoms of this syndrome can last up to eight weeks if not treated, but usually, disappear on their own after that time. It’s relatively rare for this condition to leave behind any lasting neurological damage.
Testing for Tolosa-Hunt Syndrome
Tolosa Hunt syndrome is a painful disorder that affects the eye movements. This is often detected based on the patient’s symptoms, brain scans, and response to steroid treatments. Sometimes, lab tests and examinations of cerebrospinal fluid (fluid found in your brain and spinal cord) can help rule out other causes of difficulty controlling eye movements. A tissue biopsy can also confirm the diagnosis, but it is usually not performed due to the risks and complexities involved.
The International Headache Society sets out certain criteria to aid in diagnosing Tolosa Hunt Syndrome. According to these criteria, the disorder is usually characterized by a headache that is felt more on one side, swelling in the cavities within the eyes observed on an MRI scan or biopsy, and paralysis or weakness of the eye muscles. The paralysis of eye muscles usually occurs within two weeks after the onset of headaches. Other than these, there should be no other reasonable explanation for the symptoms.
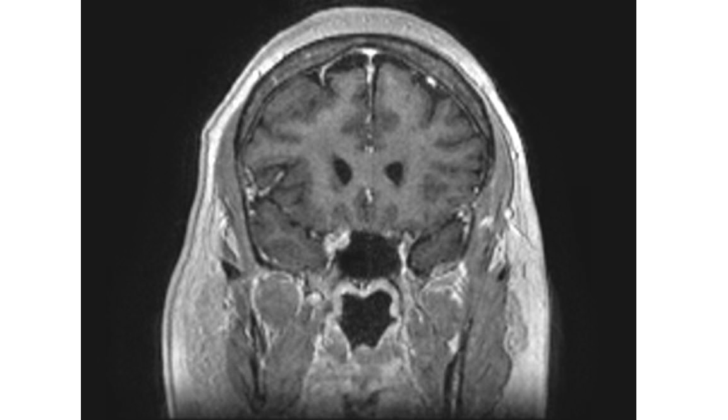
Medical imaging plays a critical role in diagnosing this syndrome. Particularly an MRI scan can help rule out other diseases that cause similar symptoms. The images often show abnormal soft tissue in certain regions of the brain which cause problems with eye movements. Other imaging techniques, such as High-resolution computed tomography (HRCT) can also be used, but MRI is preferred due to its superior visualization capabilities. MRI scans may pick up other abnormal signs, like changes in blood vessels in the brain which may help confirm the diagnosis.
When Tolosa Hunt Syndrome is suspected based on a patient’s symptoms and their MRI scan, blood tests and examination of cerebrospinal fluid can be done to rule out other possible diseases. These tests typically show normal results if the person has Tolosa Hunt syndrome. If the results are unusual, then the doctor might consider other potential diagnoses.
Treatment with high doses of steroids often leads to a dramatic improvement in patients suffering from this syndrome. Symptoms start to ease within a few days. The functioning of the cranial nerve controlling eye movement improves, and the abnormal soft tissue observed during an MRI scan reduces over the following few weeks of the treatment. However, a word of caution is necessary here as both symptom improvement and improvements seen on the follow-up brain scans can also occur with other diseases such as cancer, infection, or blood vessel diseases.
Treatment Options for Tolosa-Hunt Syndrome
Glucocorticoids, a type of steroid medication, have long been the primary treatment for Tolosa Hunt Syndrome. However, there is no specific guidance on the dosage, duration or method of administration for these steroids. It’s possible for symptoms of this syndrome to go away on their own. While steroids can greatly improve orbital pain (pain in the eye socket), there’s no proven evidence that they speed up the recovery of cranial nerve palsies, a condition where certain nerves in your head are not working properly.
The treatment plan for Tolosa Hunt Syndrome typically involves providing the patient with a high dosage of glucocorticoids initially, then slowly decreasing the dosage over several weeks or months. How quickly and by how much the dosage is reduced depends on the patient’s recovery progress. To track the progress, medical imaging like an MRI scan can be done, although the improvements in symptoms might be seen before they’re noticeable in the scans.
Only a very small number of patients may require additional immunosuppressive drugs, either to mitigate the side effects of long-term steroid use or to suppress the disease in the long run. Some of these additional drugs may include azathioprine, methotrexate, mycophenolate mofetil, cyclosporine, or infliximab. There have been cases where radiotherapy was used as a second-line treatment, especially for patients with recurring symptoms or who cannot take steroids. Usually, these patients would have a confirmed diagnosis of Tolosa Hunt syndrome, via a biopsy, before a second-line treatment is initiated.
Patients with Tolosa Hunt Syndrome usually start to feel better, especially in terms of pain relief, within 24 to 72 hours after starting steroid treatment. Typically, most patients report symptom improvement within a week. Gradually, over two to eight weeks, cranial nerve palsies might also recover. It’s rare for symptoms to persist after steroid treatment.
About 40% to 50% of patients experience a recurrence of symptoms, which can affect either one or both sides of their body. This is more common in younger patients compared to older ones. Each recurrence of symptoms should be properly investigated, as Tolosa Hunt syndrome is a diagnosis made by ruling out other health conditions. It is unclear whether steroid treatment helps in preventing these relapses.
What else can Tolosa-Hunt Syndrome be?
- Anisocoria (unequal pupil size)
- Benign Skull Tumors (non-cancerous growths in the skull)
- Brain Mets (cancer that has spread to the brain)
- Cavernous Sinus Syndromes (problems affecting the veins at the base of the skull)
- Cerebral Aneurysms (abnormal bulging in the brain’s blood vessels)
- Cerebral Venous Thrombosis (blood clot in the brain’s veins)
- CNS Whipple Disease (a rare infectious disease affecting the nervous system)
- Diabetic Neuropathy (nerve damage caused by high blood sugar)
- Epidural Hematoma (bleeding between the skull and the outer layer of the brain)
- Lyme Disease (an infectious disease usually spread by ticks)
- Meningioma (a tumor that arises from the meninges, the membranes that surround the brain and spinal cord)
- Migraine Headache (severe headache often accompanied by other symptoms)
- Neurosarcoidosis (inflammation of the brain or spinal cord caused by sarcoidosis, a disease that affects multiple organs)
- Pediatric Craniopharyngioma (a rare brain tumor mostly diagnosed in children)
- Polyarteritis Nodosa (a disease that causes inflammation of small and medium-sized arteries)
- Primary CNS Lymphoma (a type of cancer originating in the lymphatic system of the brain and spinal cord)
- Primary Malignant Skull Tumors (cancerous growths that originate in the skull)
- Systemic Lupus Erythematosus (an autoimmune disease wherein the body’s immune system attacks its own tissues and organs)
- Tuberculous Meningitis (a severe form of tuberculosis that affects the membranes covering the brain and spinal cord)
- Varicella Zoster (a virus that causes chickenpox and shingles)











