Overview of Mechanical Aortic Valve Replacement
A mechanical aortic valve replacement (MAVR) is a vital surgery for individuals suffering from serious aortic valve diseases. The aortic valve helps control the blood flow from your heart to the rest of your body. If something is wrong with it, such as aortic stenosis (narrowing of the valve) or regurgitation (the valve fails to close properly, causing the blood to flow backward), a MAVR surgery might be needed.
During the procedure, a mechanical artificial valve, built to mimic the job of the original valve, is surgically placed. A primary advantage of this mechanical valve is its durability- often outlasting biological valves (valves taken from animals or human donors) by lasting around 20 years.
Since doctors started performing aortic valve replacements back in the 1960s, there have been many improvements in the design of the valve, the surgical procedures, and the care given after surgery. All these advancements have improved the success rate of these surgeries.
Mechanical valves are often the preferred choice for certain patient groups mainly due to their longevity. They usually last longer than biological valves, which can wear out over time. Young patients or those who can handle lifelong blood-thinning medication may benefit from a mechanical valve due to its long-lasting nature, minimizing the chance of needing another surgery. However, one significant challenge is the requirement of lifelong anticoagulation (blood-thinning) therapy, which can increase the risk of excessive bleeding. Deciding whether to go for a mechanical valve involves a lot of factors including the patient’s age, lifestyle, the risk of re-surgery, and their ability to handle lifelong blood-thinning medication.
Both healthcare professional teams and patients need to consider these factors to make the most beneficial decisions. Keep in mind that the main goal is to have the best possible results from the procedure.
Anatomy and Physiology of Mechanical Aortic Valve Replacement
MAVR (Mechanical Aortic Valve Replacement) is a surgery where a diseased or malfunctioning aortic valve in the heart is replaced with a mechanical one. For this procedure to be successful, it’s important to understand the detailed structure of the aortic valve and the heart.
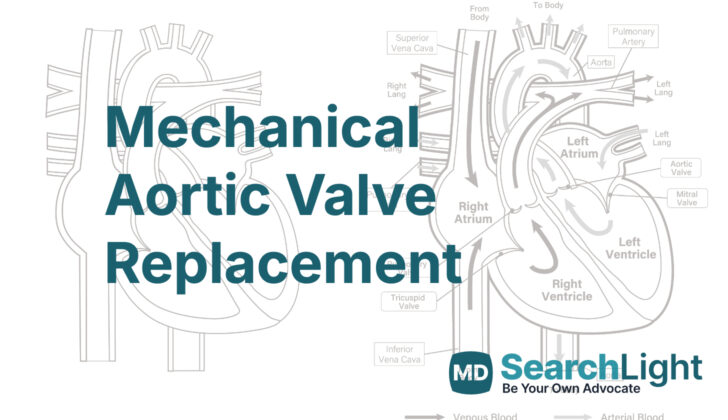
The aortic valve is a crucial part of the heart, acting like a door between the left ventricle (the main pumping chamber of the heart) and the aorta (the big pipe that carries oxygen-rich blood from the heart to the rest of the body). This “door” usually has three flaps, or ‘cusps’ – right, left, and noncoronary. These flaps open and close to regulate the blood flow, ensuring that blood only travels in one direction, from the heart to the rest of the body. Sometimes, the structure of the aortic valve may differ, such as having only two flaps, and this can complicate MAVR surgeries.
The flaps or ‘cusps’ on the aortic valve are essential in sealing and controlling blood flow from the heart. In the standard three-flap valve, the noncoronary cusp is usually the largest and handles most of the blood flow. The cusps have a critical role in making sure the valve works effectively, including creating a spherical shape with the aortic walls to maintain its function.
The ‘annulus’ is a circular, fibrous ring that acts as the foundation for the aortic valve, helping to provide stability. The mechanical prosthesis used in MAVR is anchored to this structure. This annulus also helps determine the size and position of the mechanical valve.
There are three dilated pockets within the aortic root located above the valve flaps, known as the sinuses of Valsalva. These pockets have a critical role in helping the coronary blood flow and keeping the valve function correct. The right and left pockets each contain the beginnings of the right and left coronary arteries, which are the main blood vessels supplying blood to the heart. The floor of these pockets is made up of a thin connective tissue and an area of tissue from the ventricle (the heart’s main pumping chamber).
The cusps of the valve attach to the aortic wall at areas known as ‘commissures’. These are critical for the valve’s stability and function. Structures beneath these attachments, the so-called ‘interleaflet triangles’, contribute to the valve’s structural stability and ensure one-way blood flow.
The ‘sinotubular junction’ is the boundary between the aortic root and the ascending aorta (the big blood vessel that carries blood from the heart to the body). This junction is vital in maintaining the geometry and overall function of the valve.
The left ventricle is the main pumping chamber of the heart, pushing oxygen-rich blood into the body through the aortic valve. Both the positioning and alignment of the mechanical valve are vital to ensure efficient blood flow and to minimize the risk of complications.
The ascending aorta is the part of the aorta that straight after the aortic valve. This and the coronary arteries, which provide blood to the heart muscle, are fundamental to the functioning of the heart. Care must be taken during surgery to avoid obstructing these arteries.
Why do People Need Mechanical Aortic Valve Replacement
MAVR, or mechanical aortic valve replacement, is a surgical procedure for patients with a specific heart condition known as aortic valve disease. This condition gets more common as people age and affects about 1 in 8 people who are 75 or older. MAVR is normally suggested when the patient’s original valve isn’t working correctly and needs to be replaced. This often happens because of conditions like aortic stenosis, aortic regurgitation, and certain heart defects present from birth.
Doctors decide whether a mechanical valve is right for a patient based on factors like their age, expected lifespan, the need for long-term use of blood thinners, and their general lifestyle. Some of the reasons to perform a MAVR are severe aortic stenosis, aortic regurgitation, or a congenital bicuspid aortic valve (a birth defect where the aortic valve only has two leaflets instead of three). It may also be required if a previously installed artificial valve has failed.
Aortic stenosis is a serious heart condition where the aortic valve becomes narrow, slowing down the blood flow from the heart to the body. The most common cause of this condition is aging-related changes like calcification and atherosclerosis (hardening of arteries). The symptoms of this condition may not appear until the valve becomes critically narrow. Once the symptoms like chest pain, shortness of breath, or fainting start appearing, the condition can become life-threatening. In severe cases, MAVR might be recommended even if no symptoms have appeared yet. Using tests like an echocardiogram (a type of ultrasound), doctors can decide when surgery is necessary.
Aortic regurgitation is another heart condition where the aortic valve doesn’t close properly, and the blood leaks backward. MAVR can be recommended for these individuals if they are showing symptoms or if an ultrasound shows that their heart’s left chamber is not pumping blood correctly. This condition can be mild to moderate in most cases, but continuous monitoring is required to catch any changes.
Some people are born with a disease of the aortic valve known as the bicuspid aortic valve, where the valve has only two leaflets instead of the usual three. These patients may eventually need a MAVR. Similarly, someone born with a complex heart condition might need this surgery as part of a large treatment strategy.
Lastly, MAVR might be required for patients who previously had a valve replacement using a biological valve (made from animal or human tissue) but the valve failed. Younger patients or those with a history of failed biological valves may prefer MAVR as mechanical valves are more durable and less likely to need replacement.
Patient’s age, expected lifespan, their ability to manage long-term use of blood thinners and their lifestyle play a vital role in deciding if they should receive a mechanical valve.
When a Person Should Avoid Mechanical Aortic Valve Replacement
The medical procedure known as MAVR, which is used to treat serious problems with the aortic valve in the heart, may not be appropriate for every patient. Some people may have health conditions or personal factors that might make this type of surgery too risky or not effective. These factors are sometimes referred to as ‘contraindications’ and can be split into absolute contraindications and relative contraindications.
Absolute contraindications are conditions where MAVR is usually not recommended:
Firstly, a major requirement of MAVR is the need for long-term blood thinning, also known as anticoagulation therapy, to avoid blood clots after the procedure. Patients who cannot follow the necessary blood-thinning plan, have previously shown difficulties sticking to medical prescriptions, or who refuse to take blood-thinning medications are at a higher risk of developing clots in their heart valve. An alternative might be a different type of valve that doesn’t typically require long-term blood thinning.
Secondly, if you have an ongoing infection, especially an infection of your own heart valve (a condition known as endocarditis), doctors will usually postpone MAVR until the infection is completely resolved. This is because an untreated infection can endanger the newly placed valve, resulting in serious health risks.
Lastly, if you have a severe disorder that increases your risk of bleeding, such as hemophilia, low platelet count, or similar conditions, MAVR might not be suitable for you. Since MAVR requires long-term blood thinning which can increase the chance of bleeding, the likelihood of life-threatening bleeding complications makes the procedure too dangerous.
There are also some relative contraindications, which means that while these conditions don’t always prevent MAVR, they may make the procedure riskier or less effective:
Firstly, being older or weak/fragile can lower your body’s ability to withstand long-term blood thinning treatment that comes with MAVR. Additionally, if you’re not likely to live for much longer due to other health conditions, the surgery might do more harm than good. A different type of valve that typically requires less or no long-term blood thinning might be considered instead.
Secondly, if you have serious multiple health issues such as severe kidney, liver disease, or lung blood pressure problems, the risks of MAVR surgery and necessary blood thinning might outweigh the benefits. Again, another type of valve may be a suitable alternative, or a nonsurgical method might be chosen.
If you’re pregnant or planning to become pregnant in the future, MAVR may pose risks. Blood thinning medication needed after MAVR can harm your baby and interfere with pregnancy. An alternative type of valve that requires less or no blood thinning might be a safer choice.
If you’ve had a blood clotting event in the past despite using sufficient blood thinning medication, MAVR could pose a high risk. The likelihood of experiencing another clotting event with a mechanical heart valve could be too great, so different treatments might be considered.
Equipment used for Mechanical Aortic Valve Replacement
To perform the MAVR procedure, which is a surgery that repairs or replaces the mitral valve in your heart, your doctor will need a specific set of tools and equipment. Here’s what they’ll use:
* A cardiopulmonary bypass machine – This is a device that temporarily takes over the function of your heart and lungs during the surgery. It allows your heart to be still while the doctor operates.
* Valve prostheses of various sizes – These are artificial valves that can replace your faulty mitral valve. They come in different sizes to fit different patients.
* Transesophageal echocardiography – This is a type of ultrasound that creates detailed pictures of your heart. It helps the doctor get a clear view of your mitral valve and guide the surgery.
* Surgical instruments – These are the general tools that doctors use during any surgery, like scalpels and forceps.
Who is needed to perform Mechanical Aortic Valve Replacement?
Before a heart-related medical procedure takes place, a team of diverse heart specialists comes together to assess and ready the patient. This heart team is composed of:
* A cardiologist and an interventional cardiologist – these are doctors who specialize in diagnosing and treating conditions related to the heart and blood vessels.
* Cardiothoracic surgeons – these are doctors who perform surgery on the heart, lungs, and other organs in the chest.
* A cardiac anesthesiologist – a doctor who specializes in giving medicine that either numbs a specific area of the body or puts the patient to sleep to avoid any pain during the surgery.
* Nurses – healthcare professionals who provide care, administer medication, and monitor the patient’s vital signs.
* A coordinator – a person who helps to organize and manage the entire process.
* An intensivist – a medical doctor specializing in the care of critically ill patients, usually in the Intensive Care Unit (ICU).
When it comes to performing an aortic valve replacement, which is a surgery to replace a vital valve in the heart, a team is assembled. This includes the following staff:
* A cardiothoracic surgeon – the surgeon who will be leading and performing the procedure.
* A cardiac anesthesiologist – to ensure the patient is comfortably and safely sedated during the operation.
* A perfusionist – this medical professional operates the special machine that takes over for the patient’s heart and lungs during the surgery, ensuring the body’s supply of oxygenated blood remains steady.
* Nurses – to provide assistance and care before, during, and after the operation.
* An industry representative – they are usually present when new or technologically advanced valves are used. They can provide technical expertise about the specific product.
How is Mechanical Aortic Valve Replacement performed
Aortic valve replacement is a procedure that helps patients with serious issues related to the aortic valve in the heart by improving their chances of survival. This involves replacing the damaged valve with a new, artificial one. There are two different techniques used for this procedure: surgical aortic valve replacement (SAVR) and transcatheter aortic valve replacement (TAVR).
Let me break that down a bit. In a traditional surgical aortic valve replacement or SAVR, the chest is opened to reach the heart and the damaged valve is taken out and replaced. SAVR can be performed in various ways, including using smaller incisions (minimally invasive SAVR), making an incision in the front right of the chest (right anterior minithoracotomy), making a smaller cut down the middle of the chest (ministernotomy), or a larger incision down the center of the chest (conventional sternotomy and valve replacement).
On the other hand, a TAVR involves using a small tube to replace the valve without the need for a big incision. TAVR is typically recommended for patients not suitable for the traditional surgery due to certain health risks. Different types of specialized valves are available that can be inserted into the heart using this method.
The artificial heart valves used for replacement can also vary. The three main types include mechanical, bioprosthetic, and tissue-engineered valves. Mechanical valves are made with durable materials, bioprosthetic valves are made from animal tissue or flexible material while tissue-engineered valves are developed in a lab using human cells.
The specific method used to replace the aortic valve varies according to the patient’s health and suitability for a particular surgery. In SAVR, this involves opening the chest, cooling down the body, stopping the heart, removing the damaged valve and then inserting a new one. After the new valve is put in, the heart is started again and the chest is closed.
While in TAVR, a small cut is made in the groin and the new valve is placed using a long, thin tube. The doctor watches on a screen as they guide the tube to the heart and into the valve’s location. Once there, the valve is expanded and begins to work immediately. The tube is then removed and the cut is closed.
Possible Complications of Mechanical Aortic Valve Replacement
Having surgery to replace the aortic valve, or MAVR, is a procedure that can save the lives of individuals with severe issues with their aortic valve. However, this procedure can come with various complications that need to be carefully handled. We can divide these problems into three groups: issues that show up just after surgery, issues that show up after a long time, and problems related to the blood-thinning medication needed after the surgery.
Problems Just After Surgery
Bleeding: This is the most frequent problem as the blood-thinning medication is needed. If the bleeding after the operation is severe, a second operation might be needed. This is a leading cause of health issues shortly after the surgery.
Thromboembolism: Even with blood-thinning medication, a blood clot can form on the replacement valve. This can lead to blockages in the bloodstream, like a stroke or a blockage affecting the whole body. Replacement valves that are mechanical are more likely to have problems with blood clots and bleeding because of the long-term need for blood-thinning medication to avoid blockages.
Paravalvular leak: Sometimes, a bit of blood can leak around the valve, between the ring that keeps the valve in place and the original heart tissue. If this gets too severe, it can lead to the destruction of red blood cells, heart failure, or the need for another operation.
Infection: An infection in the replacement valve, or prosthetic valve endocarditis, is a serious issue that can happen just after surgery or a long time after. It requires quick treatment with antibiotics, and sometimes a second operation might be needed.
Problems After A Long Time
Structural Deterioration: Unlike bioprosthetic valves, mechanical valves are made to last a lifetime. But, the mechanical parts can wear out over time, leading to the valve not working properly—though this is very rare.
Valve thrombosis: Mechanical valves are more likely to have blood clots, especially if the level of blood-thinning medication isn’t high enough. A blood clot in the valve can lead to a quick blockage in the valve, which needs immediate surgery.
Hemolysis: As blood cells pass through the mechanical valve, they can get damaged, leading to anemia, a condition in which there’s a lower than normal amount of red blood cells. Mild anemia is common, but severe cases might need more treatment. Blood tests usually show anemia in patients with mechanical aortic valves.[22]
Problems Related to Blood-Thinning Medication: Patients will need to take blood-thinning medication for the rest of their lives to prevent blood clots. But, this increases the risk of bleeding problems like brain hemorrhages, bleeding in the gastrointestinal tract, and other bleeding events. Balancing the prevention of clotting and avoiding too much bleeding is an important challenge.
Challenges Related to Blood-Thinning Medication Management
Patients with mechanical valves will need regular checks of their INR, a test that measures how fast the blood clots, to make sure that the blood-thinning medication is working the way it’s supposed to (usually INR 2.5-3.5 for aortic valve replacements). Any changes can lead to either blood clot or bleeding problems.
Certain medications, foods, and alcohol can interact with the blood thinner warfarin, making it difficult to consistently control the INR. Patients and healthcare professionals need to be careful with managing this.
Being pregnant while taking blood-thinning medication can be difficult as warfarin can cause birth defects and alternative blood thinners like low molecular weight heparin must be used, which requires close monitoring.
What Else Should I Know About Mechanical Aortic Valve Replacement?
MAVR, or Mechanical Aortic Valve Replacement, is a crucial, potentially lifesaving procedure for people with severe aortic valve disease, like aortic stenosis or aortic regurgitation. This is when the valve leading to your large blood vessel called the aorta stops working properly. Let’s discuss why this procedure is so important:
Durability and Longevity
MAVR involves the use of mechanical valves, which are artificial valves that take over the duty of your faulty aortic valve. One key advantage of these man-made valves is that they are robust and can last several decades. This feature is especially beneficial for younger patients who have many more years ahead of them. Unlike ‘bioprosthetic’ (made from human or animal tissue) valves, which usually last between 10 to 20 years, mechanical valves minimize the chance of needing multiple surgeries, reducing the risks that accompany repeat operations.
Restoration of Blood Flow
MAVR restores a person’s normal blood flow by swapping out the faulty valve. This allows for smooth blood flow from the heart’s lower left chamber (the left ventricle) into the aorta. This change can reduce symptoms like shortness of breath, fatigue, chest pain, and fainting, significantly enhancing the quality of life and ability to exercise for those suffering from severe aortic valve disease.
Improved Survival
Severe aortic stenosis, a condition where the aortic valve narrows, causing it to not open fully, has a high mortality rate if left untreated. MAVR can dramatically increase survival rates by treating the root cause of heart failure and lowering the risk of sudden death from a heart condition. This procedure plays a critical role, especially for patients with severe aortic stenosis, where around half of patients pass away within two years of experiencing symptoms without intervention.
Risk of Blood Clots
Importantly, having a mechanical valve means you’ll need to take blood-thinning medication for life to prevent blood clots. Mechanical valves can make clot formation more likely, and without blood-thinners, patients carry the risk of the valve getting blocked by a clot and systemic embolization – where a clot moves to another part of your body – including stroke. This situation needs careful management of blood-thinning therapy, usually with a medication called warfarin, striking a balance against the risk of severe bleeding.
Deciding Who Gets the Procedure
Deciding between a mechanical valve and a bioprosthetic valve is influenced by several factors, including a patient’s age, lifestyle, and ability to keep up with blood-thinning therapy. Younger patients usually get the nod for a mechanical valve because of its longer-lasting nature, while an older patient or those with a higher bleeding risk might be more suitable for a bioprosthetic valve. Making this decision is crucial and involves a team approach with different health professionals.
Procedure Risks
Although MAVR has tremendous benefits, it does come with risks like bleeding, infection, and the potential for the artificial heart valve not working properly. Taking blood thinners for life increases the chance of significant bleeding, which can be deadly. Additionally, mechanical valves may break down, although this is less common compared to bioprosthetic valves.
Better Quality of Life
For many patients, MAVR brings significant relief from symptoms and an improved quality of life. With the normal functioning of the aortic valve restored, patients can often return to daily routines and maintain a level of physical activity that was previously impossible due to their symptoms.











