Overview of Minimally Invasive Aortic Valve Surgery
Aortic valve replacement is the best treatment way for serious cases of aortic stenosis or aortic insufficiency. Aortic stenosis is when the aortic valve gets narrow, and aortic insufficiency refers to a situation where the aortic valve doesn’t close tightly enough. These conditions can put unnecessary strain on the heart, which can be remedied by replacing the faulty valve.
In the past, this procedure was carried out by opening up the chest through an incision along the center of the patient’s sternum, which is the bone that runs down the middle of the chest. This approach, however, had some downsides, particularly for patients with certain conditions like osteoporosis and diabetes. The sternum or breastbone of such patients is thinner and may take a long time to heal properly, leading to prolonged discomfort.
Newer, less invasive methods of performing aortic valve replacements have been developed. Instead of the large cut down the center of the chest, these procedures use a smaller incision and special tools. Apart from less scarring, benefits of these less invasive approaches include a quicker recovery period, less pain after the operation, and a faster return to everyday activities. They also result in shorter stays in the hospital overall including the intensive care unit.
While these minimally invasive methods offer several advantages, they come with a downside of their own. These techniques require the use of expensive one-time-use equipment, which can make them more expensive than the traditional surgical approach.
Anatomy and Physiology of Minimally Invasive Aortic Valve Surgery
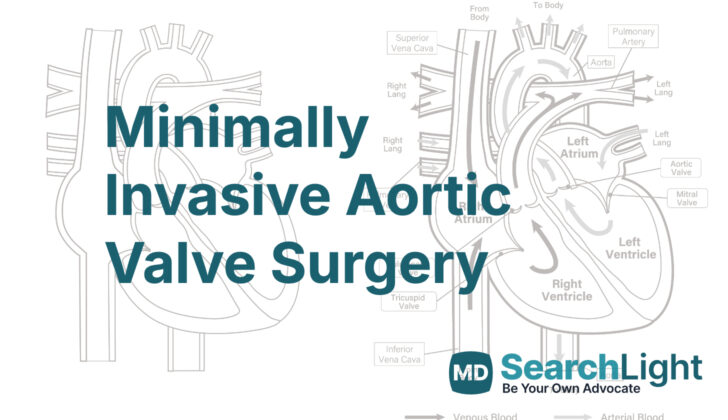
The human heart has four important valves that help control the flow of blood in and out of the heart muscle. These are the pulmonic and aortic valves, known as semilunar valves, as well as the mitral and tricuspid valves, known as atrioventricular valves. Each of these heart valves, except for the mitral valve, has three flaps or ‘leaflets’ and are surrounded by tough, fibrous rings for support.
The aortic valve is located in the middle of the large artery carrying blood from your heart to your body (ascending aorta) and the path blood takes out of your heart’s main pumping chamber (left ventricular outflow tract). This valve is positioned closely to other parts of the heart muscle, including the mitral valve at the back and to the side, the pulmonic valve in the front, and the tricuspid valve towards the back and middle of the heart.
There are three cavities or ‘sinuses’ above the aortic valve flaps separating the ‘aortic root’ (the initial part of the aorta) from the left pumping chamber of the heart. Another structure, known as the sinotubular junction, divides the aortic root from the part of the aorta that carries blood up and away from the heart.
Most people have a three-flapped aortic valve, but about 1-2% of people have an aortic valve with two flaps (bicuspid), which can sometimes cause the valve to become narrow or leaky. Normally, during the heartbeat phase when your heart is pumping (systole), the flaps of the aortic valve open and move upwards towards the sinuses. When your heart rests between beats (diastole), the valve flaps close. The design of the structure helps to prevent blocking the openings (ostia) of the arteries that supply blood to the heart (coronary arteries). Importantly, this design allows space for blood flow between the valve flaps and the wall, which helps the valve to open and close.
The size of the open aortic valve, which is measured during the pumping phase of the heart, is an important factor in understanding how well the valve is working.
Why do People Need Minimally Invasive Aortic Valve Surgery
According to the 2020 guidelines by the American Heart Association and the American College of Cardiology, there are several instances when a medical procedure to replace a valve in the heart, known as aortic valve replacement, might be suggested:
1. If you have significant, symptomatic narrowing of the aortic valve, a condition known as aortic stenosis. Symptoms may include chest pain, fainting, or heart failure.
2. Even if you don’t have symptoms but you have severe aortic stenosis and your heart is not pumping blood as effectively as expected (a condition doctors refer to as a left ventricle ejection fraction or LVEF of less than 50%).
3. If you don’t have symptoms but you have severe aortic stenosis and you are already having heart surgery for another reason.
4. If you have a severe aortic stenosis with reduced blood flow and your heart is not pumping blood as effectively as expected (a condition medically known as low flow, low gradient severe aortic stenosis with reduced LVEF).
5. If you have severe aortic stenosis with reduced blood flow but your heart is pumping blood normally, and the aortic stenosis is causing symptoms.
For a patient who has no symptoms but has severe aortic stenosis and a low risk for surgery, the following may also indicate that an aortic valve replacement is needed:
1. You become physically tired more easily or your blood pressure drops significantly during exercise.
2. You have very severe aortic stenosis.
3. Your B-type natriuretic peptide, a substance found in the blood that increases when heart failure gets worse, is higher than three times the normal level.
4. The speed of blood passing through the aortic valve increases dramatically over a year.
Patients with severe aortic stenosis without symptoms who have a progressive decrease in LVEF on at least 3 imaging studies might also need an aortic valve replacement. Similarly, if you are already having heart surgery for another reason and have moderate aortic stenosis, replacing the aortic valve might be suggested.
Surgery may be the best way to replace the aortic valve if you are younger than 65 or expected to live more than 20 years, if the structure of your heart doesn’t allow for a non-surgical approach to replace the valve or if you have no symptoms but abnormal exercise stress test, severe aortic stenosis, rapid progression, or elevated B-type natriuretic peptide.
When a Person Should Avoid Minimally Invasive Aortic Valve Surgery
There are a few cases in which a less invasive way of fixing a heart valve, or minimally invasive aortic valve replacement, might not be the safest option for a patient:
– Having serious chest wall deformities can present obstacle. For instance, having a seriously shifted heart and critical large blood vessels in the chest can make accessing the heart valve risky. Also, a deformity can make the chest wall more rigid, which can make it harder to open the chest during surgery. Pectus excavatum, a condition where the chest appears sunken or hollow, is an example of such deformity. Doctors usually use something called Haller index, which compares the width of the chest to its shortest front-to-back distance, to determine how serious the deformity is. If the Haller index is more than 3.2, it’s generally considered as a serious deformity.
– If a person has had a pneumonectomy (a surgery where a lung is removed), a less invasive heart valve replacement may not be the best option. Previous lung removal can cause the heart and critical blood vessels to shift, possibly making surgery complicated and unsafe from limited exposure. The surgery may also create scar-like tissues, called pleural adhesions, which further complicate matters. People who have had a lung removed are usually at a higher chance for complications during or after surgery, and a difficult, time-consuming valve replacement procedure could increase that risk.
– While fixing the heart valve, it is important to clearly view and control the main blood vessel in the heart, called the ascending aorta and the arch of the aorta. If these structures are heavily calcified or hard, this process becomes challenging. Also, controlling the bleeding after removing the device used to control blood flow depends on good views and freedom of movement. Since these are limited in a less invasive heart valve replacement procedure, heavy calcification of the aorta makes this procedure not the best fit.
There are also a few other situations where this type of surgery needs to be handled very carefully:
– If a patient has had radiation treatment on the front of their chest, their heart and the main blood vessel might be fragile, and there might be scar-like tissue inside the chest.
– If a person has had pericarditis—where the thin sac-like membrane surrounding the heart becomes inflamed—it might be challenging to insert the tubes that help drain and control blood in veins, due to extensive scar-like tissue. Though it’s possible to solve this by putting the tubes in veins in the leg or collarbone, the patient might need more careful monitoring after the surgery and early walking around might be a bit restricted.
Equipment used for Minimally Invasive Aortic Valve Surgery
Here is a simple breakdown of the various types of aortic heart valve replacements that are currently used in surgeries:
Bioprosthetic valves (made from pig or cow tissue):
- Stented – brands like Perimount (from Edwards), Epic (from St Jude Medical), and Hancock II (from Medtronic).
- Stented, positioned above the natural valve ring – brands like Magna Ease (from Edwards), and Mosaic (from Medtronic).
- Stented, with externally mounted valve flaps – brands include Mitroflow (from Sorin), and Trifecta (from St. Jude Medical).
- Stentless – brands like Freedom (from Sorin), Toronto SPV (from St Jude Medical), Freestyle (from Medtronic), and PrimaPlus (from Edwards).
Mechanical valves (made from man-made materials):
- Regent (from St Jude Medical) – has two leaflets or opening and closing parts.
- Single-tilting disc (from Medtronic-Hall) – no longer used today.
- Caged-ball (from Starr-Edwards) – was the original mechanical valve and is only used in history books today.
- Tilting-disc (from Björk-Shiley & Pfizer) – no longer used today.
Remember, each of these valves serve the same purpose: to help control the flow of blood through your heart in the correct direction. The valve your doctor will choose for you will depend on your specific health condition and needs.
Who is needed to perform Minimally Invasive Aortic Valve Surgery?
A procedure known as a minimally invasive aortic valve replacement requires the involvement of various medical professionals. This procedure involves repairing or replacing a valve in your heart that is not working properly. The main person leading this procedure is a cardiac surgeon – a heart doctor trained to do operations.
An important member of the team is a cardiac anesthesiologist, who is responsible for putting you to sleep so you don’t feel pain during the procedure. Operating room nurses are available to assist the surgeon during the surgery and to help care for you.
Scrub nurses or techs are specialized healthcare professionals who hand the necessary instruments to the surgeon and assist in other ways during the procedure. There’s also a member of the healthcare team called a perfusionist. This professional operates the heart-lung machine that temporarily takes over the job of your heart and lungs during the procedure, to keep your blood oxygenated and flowing.
Last but not least, cardiac intensivists are doctors who specialize in providing care for patients in the intensive care unit (ICU) after heart procedures. They play a vital role in your recovery after the surgery, making sure your recovery process goes smoothly and as planned.
Preparing for Minimally Invasive Aortic Valve Surgery
Before surgery
In heart surgery, there are different ways that doctors can fix issues with the aortic valve (the valve that controls blood flow from the heart). While certain techniques require less invasive procedures, the traditional open heart surgery remains the most reliable method. Although less invasive surgeries can have benefits, they require highly skilled surgeons and the learning process can be tough. Additionally, the potential for complications that would require a switch to the traditional open-heart method adds further complexity.
It’s important that doctors understand these less invasive options. However, to decide the best approach for each patient, a team of health professionals must closely evaluate the patient’s condition, considering the pros and cons of both open and minimally invasive methods. Once the team decides that a minimally invasive method is best, the doctors should talk to the patient about their condition and what the surgery entails. The patient should understand the risks and benefits before agreeing to the procedure.
During surgery
In the operating room, the patient will be carefully placed on the operating table, and put to sleep using general anesthesia. The anesthesia can take effect in different ways, depending on the patient’s condition and needs for the procedure. For example, some require single-lung ventilation, which needs a special type of breathing tube. The patient’s heart and breathing rate, as well as blood pressure, must be monitored and managed to prevent unwanted complications during the procedure.
Doctors also prepare a central venous access, usually with a cordis (a device for quick access to major veins), and a Swan-Ganz catheter (a special tube attached to a monitor to observe heart performance). The patient’s body from the chest down to the lower extremities should be thoroughly cleaned and shielded off in a sterile manner to reduce the risk of infection.
To find out more about the patient’s heart, the surgical team might also use a transesophageal echo (TEE) probe. TEE is a type of ultrasound that provides pictures of the heart and the aortic valve which allows the surgeons to assess its condition and make any adjustments to their surgical approach. The TEE can also give doctors insights into how well the patient’s heart is pumping blood, which can affect the post-surgery care plan, especially if the patient has heart failure.
How is Minimally Invasive Aortic Valve Surgery performed
In the past several years, heart surgeons have developed new ways to reach the aortic valve when performing heart surgery. These new approaches involve making smaller incisions or using a special type of keyhole surgery to replace the valve. Truth be told, these modern methods make recovery easier, with less postoperative pain and fewer complications compared to the traditional method. Let’s learn about these methods!
Right Anterior Minithoracotomy Approach
First, you lie flat on the operating table and are given a general anesthetic, so you’re fast asleep during the operation. A small cut about 2 inches long is made on the right side of your chest, over the heart. The surgeon gently separates the muscles to reach the heart. Then, he/she checks the position of the aortic valve, the valve that controls the flow of blood out of the heart. They then inflate one of your lungs more to help reach the heart better. Meanwhile, a tube, or cannula, is inserted into your groin area to help circulate blood while the heart is stopped for the surgery. All of this is carefully monitored with an operating team and special equipment.
The next step is to stop the heart and connect it to a heart-lung machine which takes over circulating your blood. Then, they are able to replace the aortic valve with either a mechanical or biological (tissue) replacement. Once the new valve is in place and the heart is working as intended, they’ll wake you up and bring you to the recovery room. You will have a small drain tube in your chest to help clear any excess fluid after the surgery. The incision in your chest will be closed carefully and might be stabilized with a small titanium plate if needed.
Ministernotomy Approach
The ministernotomy approach is another way to perform minimally invasive aortic valve replacement. It’s similar to the minithoracotomy, but the incision is a small “j” shape in the middle of your chest, rather than on the side. This allows the surgeon to reach your heart easier, especially for those undergoing their second aortic valve replacement or for elderly patients.
You’ll be in the same position on the operating table, and after you’re asleep from anesthesia, the surgeon makes the incision on your chest. They then open the sternum (breastbone) with a special saw and retract it to reach the heart. Once they can see the heart, they circulate your blood via the heart-lung machine as before. The same steps are followed to replace the aortic valve, and then they bring you back to consciousness for recovery. Both these procedures have fewer complications and shorter hospital stays compared to traditional aortic valve replacement.
Possible Complications of Minimally Invasive Aortic Valve Surgery
After a medical procedure, there can be several difficulties you may face. Here are some possible issues that might occur:
* Bleeding – This is when there is excess loss of blood from your body, which may happen during or after the surgery.
* Heart block – This is a condition where the electrical signals that control your heartbeat are partially or completely blocked, causing an irregular heartbeat.
* Infection – An infection may occur if harmful bacteria or other harmful microorganisms enter your body.
* Endocarditis – This is an inflammation of the inner lining of your heart.
* Air embolus – An air bubble can get into your bloodstream and then move to your brain or lungs, causing seizure or stroke.
* Sudden cardiac death – This refers to the unexpected loss of heart function and consciousness, that happens suddenly.
* Calcific embolization with stroke – Small pieces of calcium that might break off within the body, travel through your bloodstream, and can lead to a stroke.
* Irregular heartbeats (Arrhythmias) – This is when your heart beats too quickly, too slowly, or in an irregular pattern.
* Valve failure – This is when your heart valves do not open enough or can close properly.
* Pneumonia – This is an infection in one or both of your lungs.
* Anesthesia complications – These are potential risks or problems that can happen before, during, or after the use of anesthesia.
Remember, doctors do their best to provide the safest procedures and prevent these problems. Discuss any concerns with your healthcare provider before surgery.
What Else Should I Know About Minimally Invasive Aortic Valve Surgery?
There are different procedures to replace the aortic valve, a crucial component of your heart that controls the flow of blood from your heart to the rest of your body. The standard way is to do it through open-heart surgery, where the chest is opened up completely. But increasingly, doctors are becoming more comfortable with less invasive approaches. These methods don’t require the chest to be fully opened and are getting results similar to the traditional approach.
While complications with these less invasive procedures can be similar to the standard method, patient recovery is generally the same as after open-heart surgery. One such minimally invasive technique is the percutaneous transcatheter aortic valve replacement. This procedure involves inserting a new valve through a small cut in the skin, and this has been studied in large clinical trials. The results of these trials show that this technique is as safe and effective as the conventional method.
However, more research is needed to understand the long-term effects of these less invasive methods over ten years or more. The increasing popularity of the transcatheter method adds more layers to comparing these approaches with the standard one. This particular topic is quite complicated and goes beyond this explanation.











