What is Necrotizing (Malignant) Otitis Externa?
Necrotizing otitis externa (NOE), despite its misunderstood term ‘malignant’, is not cancerous but it’s a quickly spreading condition associated traditionally with a high death rate. The concept of malignant otitis externa (MOE) was first mentioned by Toulmouche in 1838, and highlighted by Chandler in 1968 because of the high death rate from the infection at the time. In modern times, MOE is more appropriately called necrotizing otitis externa (NOE) reflecting its rapidly damaging effect.
NOE is a serious infection that starts in the outer ear canal (EAC), posing potential risks to life. It’s usually caused by a bacterium called Pseudomonas aeruginosa. This infection is most common in elderly people, many of whom have diabetes. The infection mainly affects the EAC, skull base, and temporal bone and might also involve certain key areas in the head and neck. The inflammation can spread through various parts of the ear, affecting areas such as the mastoid process at the back, temporomandibular joint, parotid gland, and cervicofacial spaces at the front, or the skull base in the middle.
The condition generally starts as a basic ear infection, progressing to skin inflammation, then to inflammation of the cartilage, and finally spreading to the temporal bone resulting in periostitis and, in the end, a bone infection called osteomyelitis. The complications from NOE can be severe, including nerve damage in the skull, brain abscesses, meningitis, and blood clotting in the dural venous sinus. For these reasons, healthcare workers should always be on the lookout for NOE so that treatment can start as quickly as possible.
What Causes Necrotizing (Malignant) Otitis Externa?
The main cause of NOE, a type of outer ear infection, is a type of bacteria called P aeruginosa that is often found in water and is common in people with diabetes. Other types of bacteria, like Proteus spp and Klebsiella spp, as well as some types of fungus, such as Aspergillus spp and Candida spp, have also been linked to this condition.
NOE tends to affect older adults who are mainly male and have health conditions that weaken their immune system. Having uncontrolled glucose levels or full-blown diabetes is a major risk factor; other conditions that might put individuals at risk include HIV, cancer and treatments like chemotherapy. Diabetes can contribute to NOE by affecting small blood vessels and the immune system, especially when blood sugar levels are not well controlled. Moreover, earwax in diabetic patients is often different from those without diabetes, with a higher pH and lower lysozyme levels, making the ear more susceptible to infection.
It’s noteworthy that people who are immune-compromised due to HIV or other non-diabetic causes can develop NOE at a younger age than those with diabetes. However, they are less likely to be infected with Pseudomonas but could be at a higher risk of fungal infections. Their ear examination may also reveal a lack of granulation (new growth) tissue in the ear canal, which is usually seen in cases of infection or inflammation. These patients typically face more challenging health outcomes compared to those with diabetes.
Risk Factors and Frequency for Necrotizing (Malignant) Otitis Externa
NOE, or Necrotizing Otitis Externa, is a fairly uncommon condition. Because it’s so rare, the number of recorded cases may not truly reflect how frequently it occurs. Its rate of occurrence can vary depending on the source, with some showing it happens between 0.221 and 1.19 times for every 100,000 patients. The aging population, rise in diabetes, and more NOE diagnoses may have caused these numbers to increase recently.
NOE affects all ages, but is called out as more common in people over 60. Having a weakened immune system, common in the older population, increases the risk for NOE. Diabetes mainly causes this weakened immune state for NOE patients, but cancer, chemotherapy, and HIV also contribute. This condition is more likely in males than females. Nonetheless, keeping track of its exact occurrence rate is hard because many studies on it only have a small number of patients. Although rare, NOE can show up in children and young people who don’t have diabetes or a weak immune system.
- Necrotizing Otitis Externa, or NOE, is a relatively rare condition.
- The reported rate ranges between 0.221 and 1.19 cases per 100,000 patients.
- The number of cases might have gone up due to an aging population, increased diabetes, and more NOE diagnoses.
- NOE is especially common in people over 60.
- A weak immune system, often due to diabetes, cancer, chemotherapy, or HIV, is a significant risk factor.
- NOE is more common in males than in females.
- Even though it’s rare, NOE can still affect children and young individuals who are neither diabetic nor have a weakened immune system.
Signs and Symptoms of Necrotizing (Malignant) Otitis Externa
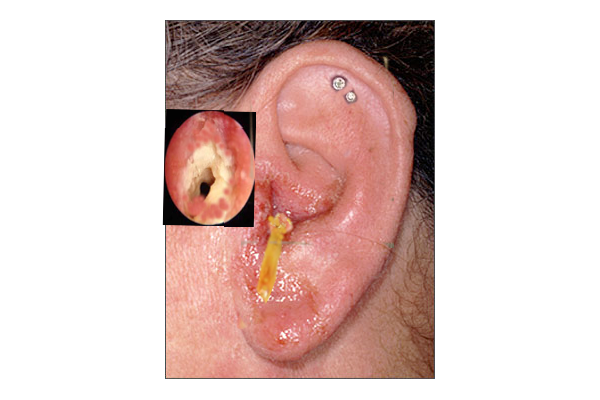
People with Necrotizing (Malignant) Otitis Externa (NOE), a severe ear infection, often suffer from an intense earache, especially at night, along with ear discharge. This doesn’t usually improve with typical ear infection treatments. In some cases, people might also display facial paralysis or other issues related to damage to the nerves around the face. A physical exam often shows a sore, red, swollen ear, and the outer ear canal might be very tender, especially between the mastoid bone (bump behind the ear) and the lower jaw. For patients where the NOE has been caused by a Pseudomonas bacteria, the appearance of granulation tissue (new connective tissue and tiny blood vessels that form on the surfaces of a wound during the healing process) at the junction between the ear cartilage and bone is a telltale sign. Fever is rare, and other vital signs are often normal.
Doctors use certain key criteria to diagnose NOE, some of which are considered ‘major’ and must all be present, while others are ‘minor’ and only need to occur occasionally. These include:
- Major Criteria:
- Pain, often more than what would be expected from a physical exam
- Swelling
- Fluid leakage from the infected site
- Granulation tissue found in the outer ear canal
- Microabscess – a small collection of pus that has formed in tissue, detected during surgical intervention
- A positive technetium-99 methylene diphosphate (Tc-99m) bone scan – a specific type of scan that is used to diagnose NOE
- No improvement even after local treatment for more than 1 week
- Minor Criteria:
- Being a patient with diabetes
- Involvement of the cranial nerves
- A positive radiograph – an image taken using radiation
- Having a debilitating condition – a disease or condition that significantly weakens or physically restricts the patient
- Being of an older age
To confirm NOE, all major criteria must be met, merely meeting minor criteria isn’t enough to make the diagnosis.
Healthcare providers should also perform a nerve examination, particularly focusing on the facial nerve, but also including nerves such as the glossopharyngeal, vagus, spinal accessory, and hypoglossal. The facial nerve is often affected due to its closeness to the back part of the bony outer ear canal. More rarely, the abducent and trigeminal nerves might also be affected, indicating a potentially poor prognosis – the likely course or outcome of the disease. It’s also important to perform a mental status examination. If there are any abnormalities, this could indicate that the infection has spread to the brain.
Testing for Necrotizing (Malignant) Otitis Externa
Blood tests are often carried out when diagnosing necrotizing otitis externa (NOE), a severe ear condition. These tests may show a normal or slightly increased number of white blood cells, and inflammation markers such as Erythrocyte Sedimentation Rate (ESR) and C-reactive protein (CRP) can be high in patients with NOE. These markers are a good way to check how well the body is responding to treatment. Blood sugar testing is also important, especially for individuals with diabetes, as NOE can affect how the body deals with sugar. Strict control of blood sugar is therefore recommended during treatment.
If there’s discharge from the ear, it should ideally be collected and tested to help guide the treatment plan. This is especially useful in instances of persistent ear infections. In some cases, a small tissue sample from the ear canal might also be required to exclude the possibility of conditions such as cancer or cholesteatoma.
Imaging techniques, such as a computed tomography (CT) scan and magnetic resonance imaging (MRI), can help provide a visual picture of the situation. CT scans are useful in showing if bones have been affected, while MRI scans are better suited to assess any impact the condition may have on surrounding soft tissues and to identify any complications inside the skull. However, it’s worth noting that both CT and MRI scans may struggle to differentiate between active inflammation and an infection that is resolving.
There are other scanning techniques too, such as the Technetium-99 bone scan, which is good for initial diagnosis but not so much for monitoring because signs of bone healing can continue to show even after the patient has clinically recovered. The Gallium-67 scan is another technique that provides more detailed tracking of the infection process than the Technetium-99 scan. It uses a radioactive tracer that is absorbed by inflammatory cells in the body, which allows doctors to see inflammation in a clearer way. There’s also the Indium-111 scan, which works similarly to the Gallium-67 scan, and the positron emission tomography connected with a CT (PET/CT) scan, which allows for the detection of metabolically active tissues.
Treatment Options for Necrotizing (Malignant) Otitis Externa
The treatment for a condition called Necrotizing Otitis Externa (NOE) involves multiple approaches. This includes the use of systemic and local antibiotics, keeping blood sugar levels under control, keeping the ear clean, and therapeutic use of oxygen under pressure (hyperbaric oxygen therapy). If these non-surgical treatments are not effective, surgery may be considered. Surgical procedures can include the removal of dead tissue, draining of abscesses, or removal of dead bone fragments.
Different types of antimicrobial (antibiotic) therapy are used in treating this condition. Commonly used topical antibiotic drops, although helpful for simple ear infections, are usually not strong enough for managing NOE and using them together with systemic antibiotics probably won’t add any extra benefits.
Before prescribing antibiotics, samples must be collected for bacterial and fungal cultures to identify the specific organism causing the infection. This step is helpful in choosing the most appropriate antibiotic treatment.
Oral ciprofloxacin, an antibiotic, can be used in uncomplicated cases, where patients can swallow pills and there are no extra complications such as cranial nerve involvement, diabetes, or severe pain requiring hospitalization. In other cases, where swallowing pills is difficult or complications are present, intravenous ciprofloxacin may be required.
Patients who are hospitalized due to severe disease or need parenteral (non-oral) therapy can begin treatment with intravenous ciprofloxacin. Once they improve, they can switch to oral medication. Or, they may continue with intravenous antibiotics delivered through a peripherally inserted central catheter (PICC) as part of outpatient care.
Systemic antibiotics are recommended for NOE treatment, selecting those that are effective against the bacteria most commonly involved, Pseudomonas aeruginosa. Fluoroquinolones, such as ciprofloxacin, are generally preferred because they infiltrate tissues effectively and orally administered, which is useful in outpatient settings.
However, the same bacteria are increasingly becoming resistant to these antibiotics, primarily due to their widespread use worldwide. So, in case of resistant organisms, the choice of initial treatment needs to be reconsidered.
If resistance to fluoroquinolones is present, other antibiotics such as ceftazidime, aztreonam, or ticarcillin/clavulanate can be used, alone or in combination with aminoglycosides, like gentamicin or tobramycin. The choice of antibiotic should be based on the specific organism, identified through culture, causing the infection. If the precise organism isn’t identified, the treatment may need to include a broader range of antibiotics to cover different types of bacteria and fungal infections.
For fungal infections, usually amphotericin B is the first choice, but itraconazole and voriconazole, with fewer side effects, are also effective options.
The treatment duration will depend on how the patient responds to it. Patients should be evaluated every 4 to 6 weeks with a specific type of scan, a Ga-67 scan. Follow-ups should continue for up to a year for high-risk patients, as the infection can come back.
Hyperbaric oxygen therapy, while commonly used in treating NOE, appears not to provide added benefits when combined with medication or surgical treatments.
Surgery is needed for those patients whose condition doesn’t improve with medication. The surgical procedures may include removal of dead tissue, removal of dead bone fragments, and abscess drainage. Even though surgery hasn’t been shown to improve the outcome significantly, it’s usually considered for patients with more severe disease.
What else can Necrotizing (Malignant) Otitis Externa be?
Necrotizing (malignant) otitis externa (NOE) can be mistaken for a number of other health conditions. These may include:
- Localized otitis externa (an infection of the outer ear)
- Acute diffuse otitis externa (a widespread infection of the outer ear)
- Chronic otitis externa (a long-lasting infection of the outer ear)
- Cancer of the ear canal
- Aspergillus skull-base osteomyelitis (a fungal infection that affects bones at the base of the skull)
Due to the similarity of symptoms, doctors may sometimes misdiagnose NOE as one of these other conditions. Therefore it is essential to perform thorough examinations to ensure an accurate diagnosis.
What to expect with Necrotizing (Malignant) Otitis Externa
Several elements can affect how long Neural Otitis Externa (NOE) lasts and its outcomes. For people with diabetes, the length of time they’ve had diabetes and how well the condition is managed can play a significant role. Lab test results showing high ESR (a marker of inflammation) and CRP (a protein that rises in response to inflammation) levels along with certain imaging findings may suggest a less favorable outcome for NOE. Older patients are also more likely to experience complications and have higher death rates than younger patients.
Patients are more likely to have a worse outcome from NOE if they present with any of the following factors:
– Involvement of the facial nerve
– Involvement of other cranial nerves
– Neurological involvement outside of the cranial nerves
– Extensive inflammation or swelling in the ear canal
– Symptoms in both ears
– Infection caused by Aspergillus species
It’s important to note that NOE has a high recurrence rate, between 15% and 20%. If ESR levels rise, this could suggest a recurrence of the disease. Because NOE can recur up to a year after treatment, patients should be closely monitored for a year before it is considered to be completely cured.
The good news is that due to advancements in diagnosis and treatment, the death rate for NOE has reduced dramatically – from 50-60%, down to 10-20% today.
Possible Complications When Diagnosed with Necrotizing (Malignant) Otitis Externa
Complications from NOE, or necrotizing otitis externa, typically occur when the infection spreads to nearby structures, mainly the nerves in the head. Although the facial nerve is most often affected, it can also impact other nerves. These can include the glossopharyngeal, vagus, spinal accessory, hypoglossal, trigeminal, and abducens nerves. If the infection extends beyond the ear bone and into the sphenoid bone, occipital bone, or clivus—the base of the skull—it’s called skull base osteomyelitis.
This can lead to serious brain complications ranging from mild confusion to much more serious conditions:
- Meningitis (an infection of the membranes surrounding the brain and spinal cord)
- Venous sinus thrombosis (clots in the veins that drain blood from the brain)
- Death
Preventing Necrotizing (Malignant) Otitis Externa
Patients need to understand the consequences of NOE (necrotizing otitis externa) and how they can minimize the risk factors that might make them more susceptible to this infection. One effective way to reduce the risk of NOE and to lessen the severity of the infection is by keeping their blood sugar levels under control. It’s also crucial for patients to avoid activities or environments that could expose them to harmful bacteria, like Pseudomonas spp.
For instance, it’s recommended to take steps to prevent the growth of bacteria that cause otitis externa, also known as swimmer’s ear. This is particularly important in hot and humid climates, as these conditions can foster the growth of bacteria. By taking these precautions, patients can reduce their chance of developing or worsening an NOE infection.











