
What is Morton Neuroma?
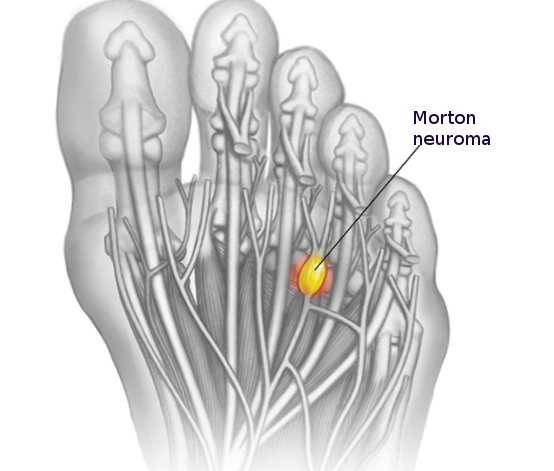
Morton’s neuroma is a condition where a nerve in the ball of the foot becomes squeezed and irritated. This typically happens due to pressure from a ligament in the foot. Despite the name, it is not a true neuroma (a type of tumor), but rather a deteriorating condition. Morton’s neuroma is also known by several other names, including Morton’s metatarsalgia, interdigital neuritis, Morton entrapment, and interdigital nerve compression syndrome, among others. The most common place for this issue to occur is between the 3rd and 4th bones of the foot, which is why it is termed Morton’s neuroma.
What Causes Morton Neuroma?
Doctors don’t know exactly why a Morton’s neuroma, a painful condition in your foot, occurs. However, they have four main theories about what might cause it.
The first is the “chronic trauma theory”, which is commonly accepted. It suggests that the action of walking can cause tiny, ongoing injuries to the nerves in the ball of your foot. These nerves become squashed between the long bones of your foot and the joints where your toes begin.
The second theory, one of the earliest proposed, is the “entrapment theory”. It suggests that the nerves in your foot can become trapped against ligaments and soft tissues in the foot.
The third theory, known as the “intermetatarsal bursa theory”, suggests that inflammation in small fluid-filled sacs (bursae) in the foot can compress and irritate nerves, causing them to thicken. Interestingly, Morton’s neuromas are usually found in parts of the foot where these bursae are close to the nerve bundles, but rarely where they are not.
The final theory, the “ischemic theory”, is based on findings that changes in the foot’s arteries occur before the nerves thicken.
Common risk factors for Morton’s neuroma include wearing shoes with narrow toes, high-heeled shoes that overextend the toes, having toes that are bent out of shape, inflammation of the bursae of the foot, thickening of foot ligaments, foot injuries, high-impact sports, joint problems in the foot, and fatty tumors.
Risk Factors and Frequency for Morton Neuroma
Morton neuroma is a condition often seen in middle-aged women, who are diagnosed with it five times more frequently than men. The exact number of people affected by this condition is unclear. It’s rare for both feet to be affected at the same time. However, it is common to find two neuromas on the same foot.
Signs and Symptoms of Morton Neuroma
If you’ve ever felt pain on the bottom of your foot between the bones leading to your toes (metatarsal heads) when walking or wearing tight, high-heeled shoes, it could be a common symptom of a particular foot condition. This pain might feel like burning, stabbing, or tingling, similar to electric shocks. Some people say it feels like walking on a stone or marble. Less than half of the people experiencing this also report numbness between their toes. After long periods of walking, the pain can spread to the back of the foot or even up the leg, leading to cramps. Interestingly, taking a rest and removing your shoes can often provide relief.
- Pain on the bottom of your foot, between the metatarsal heads
- The pain is worsened by walking or wearing tight, high-heeled shoes
- Pain can be described as burning, stabbing, or tingling
- Some people may feel like they’re walking on a stone or marble
- Less than half of those affected also experience numbness between their toes
- The pain may spread to the back of the foot or leg, causing cramps, after prolonged walking
- Relief can often be felt after resting and removing shoes
Testing for Morton Neuroma
Your doctor will typically diagnose your condition after discussing your symptoms and examining your foot. Pressing on the affected area might reproduce your symptoms. Squeezing your foot while feeling the affected area often results in a significant crunching or clicking sensation, commonly referred to as the “Mulder’s click.”
Some doctors may choose to further confirm their diagnosis by injecting the affected area of your foot with a local anesthetic called lidocaine. They will use a small amount of this medication. To rule out other conditions, such as deformities, arthritis, or dislocation of bones, they might also take standing x-rays of your foot. Additionally, if there is a noticeable difference of space between your toes when you are bearing weight or your toes are spreading out, this might be noted as a sign of your condition, which is referred to as Sullivan’s sign.
A foreign body, such as a piece of glass or metal, can also be detected if it shows up on an x-ray. An ultrasound scan done by a skilled radiologist can also be a useful tool for diagnosing this condition. They could also use ultrasound guidance to give a steroid injection in the same sitting. An MRI might be ordered in certain situations, especially when other foot issues need to be ruled out. This kind of imaging can show a specific soft tissue lesion within the space between the metatarsal bones of the foot. The details of this lesion, its shape, and its characteristics in response to the MRI can provide valuable information for the diagnosis. Ultrasound can also show this lesion and might even allow the Mulder’s click to be felt when the probe is used to press on the area.
Treatment Options for Morton Neuroma
If you’re experiencing pressure on a nerve in your foot, there are several non-surgical treatments that could potentially help. These include simply wearing wide, soft-soled shoes with low heels, or shoes with firm soles, as recommended by some doctors, to relieve pressure on the nerve. Certain types of foot support, like a metatarsal pad, can assist in spreading the metatarsal heads and decrease pressure on the nerve. If synovitis, which is inflammation of a joint, or even a toe deformity, is present, a Budin splint or specific toe strapping can help reduce nerve pain.
Medications like anti-inflammatories, antidepressants (such as amitriptyline), and anti-seizure drugs (like gabapentin) can be used to manage nerve symptoms. In some cases, steroid injections may help, but their effect often doesn’t last very long and they can have side effects like skin discoloration and fat atrophy, which is a loss of fatty tissue. Other less invasive treatments, like radiofrequency ablation, cryotherapy, and alcohol nerve injections have also been suggested.
If these non-surgical treatments don’t work, surgery might be necessary. One type of surgery involves removing the neuroma, or the mass in the nerve. An incision could be made at the top (dorsal approach) or bottom (plantar approach) of the foot. The dorsal approach is usually more desirable because scarring on the bottom of the foot can be painful. During the operation, the surgeon makes an incision, releases any obstructions around the nerve (tissue adhesions), and can decompress the nerve or cut and suture it to prevent a painful growth after surgery.
Post-surgery, you would wear a special shoe until the stitches are removed after one to two weeks, and a compressive wrap for two to six weeks.
A plantar incision might be used for recurrent neuromas, or when a patient has a tender trigger point for nerve pain closer to the heel of the foot. This approach provides a more direct exposure of the nerve and allows its more complete removal. However, it may cause painful scarring at the bottom of the foot and keratosis (thickening of the skin) in about 5% of cases.
What else can Morton Neuroma be?
These are some conditions that might explain foot pain:
- Stress fracture in the foot bone (Metatarsal stress fracture)
- a foot deformity where a toe curls down instead of pointing forward (Hammertoe)
- certain types of chronic joint conditions (Rheumatoid arthritis or Osteoarthritis)
- Cancer (Malignancy)
- a noncancerous lump filled with a jelly-like fluid (Ganglion cyst)
What to expect with Morton Neuroma
Conservative treatments for certain medical conditions can differ in their effectiveness. Some common approaches include changing footwear, altering physical activities, and medication usage to curb pain and reduce symptoms. Combining different strategies often works well. A careful examination of non-surgical treatment options was conducted. This looked at non-invasive solutions (like adjusting movements, wearing wider shoes and using special foot padding, using extracorporeal shockwave therapy, and different types of shoe inserts) as well as invasive methods (like corticosteroid injections, sclerosing injections, radiofrequency ablation, cryo-neurolysis, and botox injections). This analysis found the most reliable pain relief from corticosteroid injections and adjusting body movements.
Various studies explored the success rates of surgeries. One study involving 81 patients found that 45% of them experienced excellent results, and another 32% reported good results. But around 8% of patients saw poor outcomes. It’s unclear whether performing neurolysis (surgery to remove a portion of a nerve) or a neurectomy (surgery to remove a nerve) is a better option. However, one study suggested that neurolysis usually has satisfactory results. But, when the nerve is highly thickened or there’s a pseudo-tumor–a false-tumor–then a neurectomy might be the better choice.
A comprehensive review and analysis of 35 studies, involving nearly 3000 patients with Morton’s neuroma (a painful condition affecting the foot), compared several treatments: injection therapy (using both alcohol and non-alcohol), neurolysis, and neurectomy. The review revealed that after injection therapy, 43% of patients felt complete relief; 68% experienced no more pain after neurolysis, and 74% were pain-free after neurectomy.
Possible Complications When Diagnosed with Morton Neuroma
Chronic regional pain or long-lasting discomfort in a part of the body can occur following certain medical procedures. Another possibility includes a return of a deformity due to either a removal of a Morton neuroma (painful condition that affects the ball of your foot) that isn’t sufficient, or transformation of the Morton neuroma into a true neuroma (a growth or tumor of nerve tissue).
Complications related to surgery, such as infection, pain, or bleeding are also possible. Another type of complications can be associated with steroid injections, known as corticosteroids, which may cause skin or fat pad thinning (atrophy) and changes in skin color.
Possible Complications Include:
- Chronic regional pain
- Return of deformity
- Infection related to surgery
- Pain related to surgery
- Bleeding related to surgery
- Skin or fat pad thinning (atrophy) due to corticosteroid injections
- Skin color change due to corticosteroid injections
Preventing Morton Neuroma
It’s important that patients know what to expect from their treatment, and that they understand that outcomes can vary. This includes understanding that success rates can differ when it comes to physical therapy, changing one’s activities, or using suitable footwear. It’s also crucial they comprehend the role of other treatments, like injections or cold therapy. Additionally, when it comes to considering surgery, they should be aware that a small number of patients have reported experiencing more pain after their operation.











