What is Pontine Infarction?
The pons is a large part of the brainstem which is located between the midbrain and the medulla oblongata. An interruption of blood supply to the pons can lead to an ischemic stroke known as a pontine infarction. This can either occur suddenly (acute) or slowly over time (chronic).
The symptoms of a pontine infarction can vary widely. They can range from a condition called ‘crossed syndrome,’ where someone experiences nerve weakness on one side of the face, and movement or sensation loss on the opposite side of the body, to other less common symptoms like pure muscle weakness (hemiparesis), paralysis (hemiplegia) on one side only, or a pure sensory stroke which affects only the sensation.
The exact symptoms largely depend on the exact area within the pons that has been damaged by the stroke and which blood vessels were involved.
What Causes Pontine Infarction?
Pontine infarction is a type of stroke that happens in the pons, a part of the brain. It can be caused by a few different things, with the most common ones being small artery disease, large artery disease, and heart-generated clots. However, these last two conditions are less common causes.
Most of the blood getting to the pons comes from the paramedian perforating arteries and the short circular arteries, which are connected to the basilar artery, a major artery in the back of the brain. Other arteries, such as the anterior inferior cerebellar artery and the superior cerebellar artery, also contribute to the supply of blood to the pons.
The area of the stroke in the pons can happen at various places – either on one side or both sides, at the front or back, or in the middle or sides, or any mix of these regions.
The risk factors for ischemic stroke, such as high blood pressure and diabetes, are the same leading risks for a pontine infarction. If high blood pressure or diabetes has been present for a long time, it can lead to changes in the small arteries of the pons (a process called lipohyalinosis), eventually causing chronic low blood supply to the pons and a stroke.
A stroke can also happen if fatty substances (referred to as atheromatous plaques) accumulate in larger arteries like the vertebral or basilar artery limiting blood flow to the smaller arteries of the pons.
Other potential risk factors include smoking, high cholesterol, a history of heart disease that reduces blood supply, conditions causing increased blood clotting, and inflammation of the blood vessels (vasculitis). However, the specific risk factors that increase the chances of a stroke happening specifically in the pons aren’t clear.
Risk Factors and Frequency for Pontine Infarction
Pontine infarctions, or strokes that occur in a specific area of the brain called the pons, are relatively common but are often part of a larger stroke impacting the back portion of the brain. Different parts of the pons can be affected, each changing how the stroke presents itself:
- The anteromedial and anterolateral region, supplied by the basilar artery, is most often affected.
- The lateral region, which is supplied by the basilar artery and anterior inferior cerebellar artery.
- The posterior/dorsal region, supplied by the superior cerebellar artery.
In general, strokes are more common among men than women, and amongst Black and Hispanic adults compared to their white counterparts. This varies by location. However, specific research on pontine infarctions is currently not sufficient.
Signs and Symptoms of Pontine Infarction
A pontine infarction, or a type of stroke that happens in the pons area of the brain, is more commonly seen in older people who have chronic health conditions like high blood pressure, diabetes, high cholesterol, or heart disease. However, it can still occur in younger individuals if they have certain vascular disorders. Understanding when stroke symptoms began is vital for developing the appropriate treatment plan.
The specific symptoms of a pontine infarct can depend largely on which areas in the brain are affected. Here are some potential symptoms categorized into three types of infarctions:
- Ventro-caudal pontine infarction: Can cause weakness or paralysis on the opposite side of the body, difficulty moving the eyes and/or face on the same side, and decreased ability to feel pain and temperature on the opposite side of the body.
- Mid-pontine base infarction: May result in unsteadiness on the same side, weakness in the face on the same side and paralysis on the opposite side of the body. Different combinations of these symptoms can lead to various syndromes.
- Tegmental pontine syndrome: Can affect various brain areas and cause a wide range of symptoms including sensory disturbance, paralysis, impaired blinking, loss of sensation on the opposite side of the body, and unsteadiness on the same side.
Multiple pontine infarcts largely in the areas served by the perforating arteries can result in pseudobulbar palsy, causing severe difficulty swallowing and speaking. Bilateral pontine infarcts, due to poor blood flow in the main basilar artery, can result in paralysis in both sides of the body and consciousness impairments. This could lead to a severe condition known as locked-in syndrome, where individuals cannot move but are fully aware.
Some features that can help identify the location of the pontine infarction include:
- Weakness on the opposite side of the body, eye movement issues, and problems with coordinated eye movements for a medial infarction.
- Loss of sensation and unsteadiness on the opposite side of the body for a lateral infarction.
- Lower facial nerve issues, difficulty moving the eyes, loss of hearing, and dizziness for a caudal infarction.
Testing for Pontine Infarction
If you have symptoms of a stroke, the first thing that doctors will do is check your blood pressure and heart rate. They’ll also measure your respiratory function – how well your lungs are working. This is because a big stroke in a certain part of the brain (called the pons) might affect your ability to breathe, and you may need help breathing with a machine.
Once your doctors are sure you’re stable, they’ll perform a complete neurological examination. This involves several tests to check different functions of your brain. It helps your doctors figure out exactly where in the brain the stroke has happened and whether the stroke is due to a blockage (ischemic stroke) or bleeding (hemorrhagic stroke). It also helps them understand if any underlying conditions, like high blood pressure, might have contributed to the stroke.
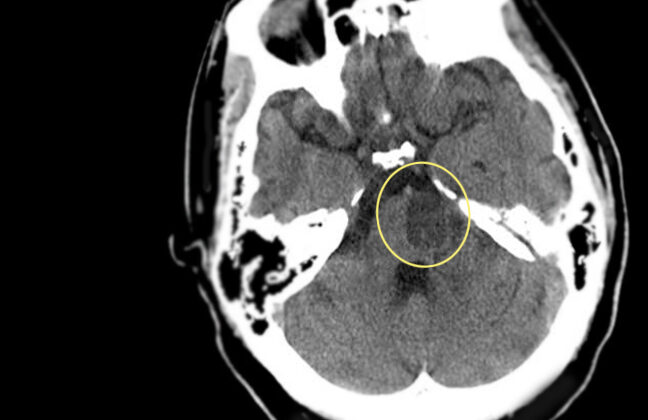
After these tests, your doctors will likely order imaging, like a CT scan or an MRI. These images can help confirm whether you’ve had a stroke and the type of stroke. The CT scan is typically the first choice because it’s widely available and can quickly show if there’s any bleeding in the brain. But the MRI can show if you’ve had an ischemic stroke, as it can detect areas of the brain that aren’t getting enough blood within minutes of the stroke happening.
Other imaging tests might be done if your doctors suspect a large artery is blocked or if they think a clot traveled from somewhere else in your body to your brain, causing the stroke. They’ll also likely order blood tests and an electrocardiogram (a test that shows how your heart is working) to get a complete picture of what’s going on with your overall health.
In the future, doctors might also be able to use specific biomarkers (substances that can be measured in the blood) to help predict how stroke patients will recover. Right now, these tests are still being studied and aren’t used regularly.
Treatment Options for Pontine Infarction
Treatment for pontine infarction, a type of stroke affecting the lower part of the brain, mainly involves steps that are common to the treatment of other forms of ischemic stroke, where the blood supply to the brain is reduced or blocked. However, due to a lack of substantial clinical evidence, therapies specifically designed to treat posterior circulation stroke, which includes the pontine infarction, might differ somewhat from those for stroke in the anterior (front) portion of the brain.
Pontine infarctions can be especially severe if caused by a blockage in a large blood vessel. In general, after determining the exact type of stroke, the treatment aims to reduce the area of brain tissue affected by lack of blood supply, prevent complications, and promote early recovery of movement and other activities. But the first priority is always to ensure the patient is stable, focusing on airway, breathing, and circulation.
Intravenous alteplase, a medication used to dissolve blood clots, is the preferred therapy for stroke patients admitted within 4.5 hours after symptoms begin. It is used as long as there are no major medical reasons against using this drug. If there is a large artery blockage, a surgical procedure called mechanical thrombectomy, which involves removing the clot causing the stroke, can be performed within 24 hours of when symptoms appear.
Patients with acute stroke typically have elevated blood pressure, which can be beneficial as it helps maintain blood supply to the brain, especially in those with large vessel occlusion. For those receiving clot-dissolving medication, it’s recommended keeping the blood pressure below 180/105 mmHg for the first 24 hours to prevent further injury due to an abrupt return of blood flow. If a patient is not receiving these medications, high blood pressure is usually not treated unless extremely high to allow blood to reach the brain despite the blockage.
Other methods to prevent further strokes include the use of anti-clotting drugs such as aspirin, clopidogrel, warfarin, apixaban, dabigatran, based on the cause of the stroke. Prescription medications to lower cholesterol levels can also help to prevent recurrence. Hypertension drugs might be added to the regimen at discharge if the patient has high blood pressure. Equally important is lifestyle modification, such as increasing physical activity, quitting smoking, modifying the diet, and losing weight if necessary.
What else can Pontine Infarction be?
An isolated pontine infarction, which is a type of stroke that occurs in the brainstem, happens less frequently than larger brainstem strokes. Common risk factors include high blood pressure, diabetes, hardening of the basilar artery, and lack of blood flow to the vertebrobasilar region of the brain. This condition can present itself with various symptoms, which makes it important to rule out other diseases.
The diseases that need to be considered include:
- Todd paralysis
- Intracranial hemorrhage
- Brain tumors or abscesses
- Spinal cord compression
- Low blood sugar (hypoglycemia)
- Wernicke encephalopathy (a serious brain disorder)
- Conversion disorder (a psychological condition)
- Complex migraine
To help determine the cause of symptoms, doctors may use neuroimaging. CT scans, which are often used to identify bleeding in the brain, and MRI scans, which are better for identifying growths, abscesses, infections, and other causes. Doctors should keep in mind less common diagnoses when examining the results.
What to expect with Pontine Infarction
The outlook for patients with a pontine infarction, which is a type of stroke that affects a part of the brain called the pons, is generally good, especially if the stroke affects only one side of the pons. This is particularly the case if the stroke is of a type known as lacunar infarction, and it affects the sides or the top-middle parts of the pons.
However, the outlook is less favourable if the stroke affects both sides of the pons or the lower part of the pons. Some patients may experience worsening neurological symptoms after a pontine infarction.
In terms of long-term outlook, one study which followed patients for 4 to 9 years after a pontine infarction found that the prognosis was generally good. Yet, another study found that the risk of experiencing another stroke in the long term was high for those who had a pontine infarction.
As for how the outlook of a pontine infarction compares to that of other types of strokes affecting the posterior circulation (the back part of the brain) or any non-pontine infarctions, it is yet to be determined.
Possible Complications When Diagnosed with Pontine Infarction
Pontine infarction is a stroke that occurs in the pons, part of the brain stem. Complications related to this kind of stroke can include:
- The most serious is aspiration pneumonia, which is often caused by pseudobulbar palsy or locked-in syndrome.
- Difficulty swallowing that necessitates tube feeding.
- Urinary incontinence that can increase the risk of urinary tract infections due to the need for catheterization.
- Residual weakness in the muscles, resulting in falls.
- Depression following the stroke.
- Complications due to being unable to move for a prolonged period, such as pressure ulcers, deep vein thrombosis, and pulmonary embolism.
Disability over the long term is also common after this type of stroke. Doctors use various scales like the Barthel Index, the Glasgow Outcome Scale, and the Modified Rankin Scale (mRS) to assess disability.
In addition, pontine infarction can lead to neurological problems such as cerebral edema (swelling in the brain), hemorrhagic transformation (bleeding within the infarcted region), palatal myoclonus (involuntary jerking of the palate), and worsening of neurological function despite treatment.
Recovery from Pontine Infarction
If someone has had a pontine infarction, which is a type of stroke that occurs in the pons region of the brain, they might need rehabilitation to recover. This could involve a number of things like sensory reeducation, which is a process where patients relearn how to perceive sensations, physical therapy to improve strength and movement, speech therapy to help with communication, and occupational therapy to support daily activities and work-related skills.
Preventing Pontine Infarction
Protecting yourself against the risk of having a stroke involves controlling risk factors that can be changed. These key risk factors include high blood pressure, diabetes, high cholesterol levels (dyslipidemia), and smoking. However, there are also risk factors that can’t be changed, such as age, race, gender, and family history of stroke. These should be taken into account as well when working to prevent strokes.
The American Heart Association and American Stroke Association have guidelines to minimize one’s risk of experiencing a stroke. They include:
- Maintaining a healthy blood pressure level. This includes regular check-ups, medication if necessary, and self-monitoring of blood pressure. The goal is to have blood pressure below 140/90 mmHg.
- Treating abnormal cholesterol levels. This means following a healthy lifestyle and potentially taking statins (cholesterol-lowering drugs), especially if you have a heightened risk of stroke. For those with diabetes, doctors recommend both taking statins and keeping blood pressure in check.
- Quitting smoking. This can be achieved through counseling and, if needed, medication.
- Adopting healthy eating habits. This can involve following diets that have been proven to help, such as the DASH diet (which includes plenty of fruits, vegetables, and low-fat dairy products), a low sodium diet, or a Mediterranean diet.
- Exercise regularly. Aim for moderate to intense workouts for around 40 minutes a day, at least 3 to 4 days a week.
- Weight reduction for those who are overweight or obese.
- Taking preventive blood thinning medication (like aspirin or warfarin) for people with a heart condition known as atrial fibrillation.
Teaching people about stroke risk factors and how to minimize them through lifestyle changes has proven to be effective. It helps individuals understand the risk and behave in ways that can reduce it. However, although people like to be informed about their chances of getting a stroke, using tools to calculate this risk doesn’t necessarily influence their behavior any more than simply teaching them about risk factors.











