What is Central Line–Associated Blood Stream Infections?
A central line-associated bloodstream infection, or CLABSI, is a term used when a harmful substance is found in a blood test from a patient who had a central line, which is a type of IV, either during the time of the infection or within two days before the infection started. Among all infections linked to health care, CLABSIs are known to be very costly, with each case roughly coming to $46,000. However, most of these infections can be prevented through proper cleanliness practices, regular monitoring, and correct management strategies.
What Causes Central Line–Associated Blood Stream Infections?
Data from the National Healthcare Safety Network (NHSN) collected between January 2006 and October 2007 has shown that various kinds of bacteria play a role in causing what’s known as central line-associated bloodstream infections (CLABSI). Most commonly, Gram-positive bacteria are to blame, with types like coagulase-negative staphylococci, enterococci, and Staphylococcus aureus taking up a large chunk. Following these are Gram-negative bacteria, such as Klebsiella, Enterobacter, Pseudomonas, E. coli, and Acinetobacter. Candida species and other types of bacteria are also contributing factors.
In the case of catheters used for long-term treatment of kidney failure, these are more likely to result in bloodstream infections. About 40-80% of these infections are caused by Gram-positive bacteria, with coagulase-negative Staphylococci, Staphylococcus aureus, and Enterococcus being the most frequent. Bacteria resistant to common antibiotics, like Methicillin-resistant staphylococcus, are often seen. And, Gram-negative bacteria cause about 20-30% of these infections.
Risk Factors and Frequency for Central Line–Associated Blood Stream Infections
Central Line-Associated Bloodstream Infections (CLABSIs) are a serious issue that leads to longer hospital stays and increased costs, while also raising the risk of patient death. Around 250,000 of these infections occur every year, most of which are associated with intravascular devices or medical equipment that’s inserted into a vein. In the U.S., Intensive Care Units (ICUs) see roughly 0.8 CLABSIs for every 1000 days a central line is in use.
Data from around the globe also makes it clear that this is a widespread issue. Between 2010 and 2015, the International Nosocomial Infection Control Consortium recorded a CLABSI rate of 4.1 per 1000 central line days across 703 ICUs in 50 countries.
Another important factor is that many central lines are in use outside of ICUs. In one study, it was found that 55% of ICU patients and 24% of non-ICU patients had a central line. In fact, the majority (70%) of hospitalized patients with central venous catheters were located outside of an ICU.
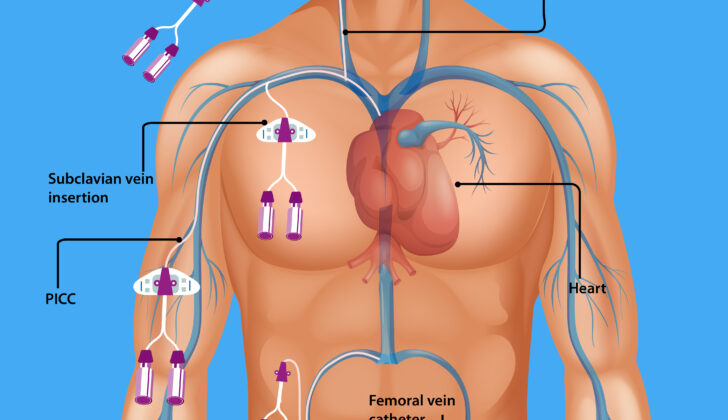
- Central venous catheters are sometimes known as Peripherally Inserted Central Catheters (PICCs).
- PICCs are becoming more popular in both ICUs and general wards.
- They offer several benefits, including quick access to the central venous system and can be easily placed at the bedside by trained nursing staff using ultrasound.
- These catheters are inserted into a peripheral vein in the arm and advanced into a central vein (either the cavoatrial junction or the right atrium).
- Despite these benefits, the rates of CLABSI associated with PICCs are similar to those seen with traditional central venous catheters (CVCs) in a hospital setting.
- In a large study of over 27,000 patients in multiple centers, no significant difference in CLABSI rates was found whether PICCs were used in an ICU or general ward.
However, this study was limited by a relatively low number of events.
Signs and Symptoms of Central Line–Associated Blood Stream Infections
The way a person feels when they are sick can change based on how severe the illness is. Fever and chills are the most common symptoms, but these might be hidden if the person’s immune system isn’t working properly or if they are very young or very old. In these situations, symptoms can show up differently. They might include changes in mental state, low blood pressure, feeling tired, or feeling weak. It’s important to check the site where a catheter was inserted for any signs of inflammation. This is done by looking at it and feeling gently along the path under the skin.
- Pain
- Swelling
- Discharge from the site
- Redness around the site or along the path under the skin
The above are what people might report if there are infections at the catheter site or along the path under the skin. For catheters that stay in place for a long time, having trouble to draw blood or slow flow can be risk factors and signs of a bloodstream infection caused by the catheter.
Testing for Central Line–Associated Blood Stream Infections
In addition to a regular physical check-up, laboratory tests play a vital role in diagnosing and managing illnesses. A blood culture, which involves testing a sample of blood for bacteria or yeast, is the first step in diagnosing any possible diseases. Other important tests include a complete blood count, serum electrolytes, and kidney and liver function tests. These tests are necessary to gauge the severity of the condition and to check for any additional diseases. When tests are being conducted, paired blood cultures must be extracted from the central line and peripheral vein, and labelled properly before sending them for analysis. If it’s hard to get a sample, then multiple samples are taken from different areas using a special device known as a multi-lumen central line.
In the process of diagnosis, there are specific terms you should be familiar with:
A Catheter-related bloodstream infection (CRBSI), also known as blood poisoning, is defined by the Infectious Diseases Society of America (IDSA) as an infection happening due to a catheter (a thin tube used to deliver medications and treatments directly into a vein). Diagnosis involves stringent processes like isolating the same pathogen from blood culture taken from both the central line and the peripheral vein. The bacterial count in the central line sample must be at least three times higher than that in the peripheral vein.
The Centers for Disease Control and Prevention (CDC) uses a surveillance term, Central Line-Associated Bloodstream Infection (CLABSI), defined as an infection stemming from a central line. The infection should not relate to any other infection the patient might have and should not be present when the patient first enters the facility.
For tunneled catheters (special tubes placed under the skin to deliver treatments), two specific definitions are critical:
Exit site infection: Signs of inflammation confined to an area (typically less than 2 cm) around the catheter exit site and any fluid that is tested and found to contain bacteria or yeast.
Tunnel infection: When inflammation extends beyond 2 cm from the exit site, usually associated with pain and tenderness along the groove under the skin and any fluid at the exit site that tests positive for bacteria or yeast. This fluid might only be visible when removed by pressing on the skin for examination.
Treatment Options for Central Line–Associated Blood Stream Infections
If there are suspicions of CLABSI (an infection caused by a central line in a vein), an immediate treatment should be started before culture test results are received. The treatment will be based on the presumed infection cause, patient’s individual factors and the overall clinical situation. Generally, it should cover common gram-positive and gram-negative bacteria. Local prevalence and resistance to antibiotics should also be taken into account. Here are some considerations:
1. If there is a high number of MRSA (a type of staph bacteria resistant to antibiotics) in your local area, then vancomycin should be administered. If not, cephalosporins or penicillins that are able to kill staph bacteria would be sufficient. When MRSA is found to be resistant to vancomycin, then daptomycin is the best alternative.
Choosing an antibiotic to treat gram-negative bacteria should take into consideration the risk of a Pseudomonas infection and what the bacteria in your local area are susceptible to. If the risk of a Pseudomonas infection is low, then ceftriaxone should be suitable. A combination of a beta-lactam (lactamase inhibitor) and an aminoglycoside can be used for critically ill patients or those who are at high risk of resistant bacteria. This combination is crucial for patients with neutropenia (low neutrophil count in the blood), a severe illness, or for those who have been previously colonized by Pseudomonas.
Echinocandins are advisable for suspected candidemia (yeast infection in the blood) patients, especially if there are reasons to suspect resistance to azole (another type of antifungal). Otherwise, fluconazole should be acceptable. Antifungal therapy should be expected in certain cases, such as when there’s prolonged administration of broad-spectrum antibiotics, a history of haematologic malignancy, or if the patient has undergone organ or bone marrow transplant.
Once the sensitivity of the bacteria to antibiotics is known, de-escalation to specific and tailor-suited treatment is advised. If bacteria is not growing in cultures, antibiotics may no longer be necessary. If a patient with a short-term catheter experiences unexplained, persisting fever or sepsis, the catheter should be removed and the tip sent for culture for a CLABSI diagnosis.
Catheters causing CLABSI should be removed quickly, especially if there are strong clinical suspicions of infection. Only in certain exceptional situations, long term catheters can be saved by pairing systemic therapy with the locking technique (heparin + high concentration of antimicrobial).
Infections around the exit site of tunneled hemodialysis catheters can be treated with a short course of both topical or systemic antibiotics. Catheters with a higher risk of infection should be removed. There are particular circumstances when a CLABSI from hemodialysis access should be removed:
1. When symptoms persist over 36 hours.
2. When the bacteria is not eliminated after 3 days of apt antimicrobial therapy.
3. When organisms are difficult to eliminate.
4. When there is recurrence of non-complicated CLABSI.
The duration of therapy for CRBSI patients differs by case. The approach for intravenous antimicrobial therapy could consider:
1. S.aureus – 14 days if there is no endocarditis.
2. Coagulase-negative staphylococci – 7 days.
3. Enterococci and gram-negative bacilli – 10 to 14 days.
4. Candida – 14 days if there is no retinitis.
What else can Central Line–Associated Blood Stream Infections be?
Types of infections that might occur in certain conditions could include:
- Infections at the point of surgical incision or exit site
- Inflammation of the veins, also known as phlebitis
- Infections in a localized area under the skin, often referred to as a ‘pocket infection’
- Widespread infection throughout the body, known as sepsis
- Infections along a passageway under the skin, termed tunnel infections
- Infections in the urinary system, referred to as urinary tract infections











