What is Brain Herniation?
Brain herniation is a serious condition where parts of the brain start to press on and move into areas they shouldn’t, due to increasing pressure inside the skull. This is often described as a “brain code,” signalling the urgent need to stop this harmful process.
The brain normally sits comfortably within the skull. However, if pressure inside the skull starts to rise, the brain’s protective fluid called cerebrospinal fluid (CSF) and the amount of blood in the brain make some room for this increased pressure under a principle known as the Monro-Kellie doctrine.
At times, the severity of the situation can surpass these protective mechanisms of the brain. Consequently, certain parts of the brain start squishing into spaces formed by natural structures within the skull, causing progressive herniation syndromes, which can be life-threatening events needing urgent care.
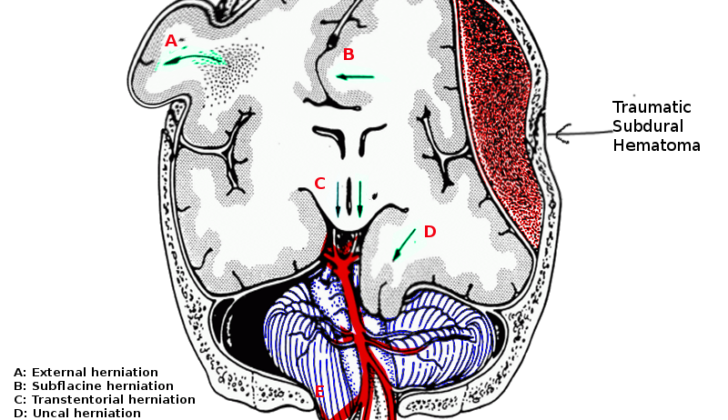
There are different types of brain herniations:
* ‘Subfalcine’ is when a part of the brain called the cingulate gyrus is pushed against a structure in the skull known as the falx cerebri.
* ‘Transtenorial’ or ‘uncal’ is when the inner part of your temporal lobe (a region of the brain) are compressed due to a mass under and across another structure known as the tentorium.
* ‘Central’ herniation occurs when both temporal lobes press through a space known as the tentorial notch.
* ‘Tonsillar’ herniation happens when a mass below the tentorium forces part of the cerebellum (a region at the back of your brain) through a large hole at the base of the skull called the foramen magnum.
* ‘Upward’ herniation is when a mass below the tentorium compresses the part of the brain that connects it to the spinal cord, known as the brainstem.
What Causes Brain Herniation?
There are many things which can put a person at risk for increased pressure in the brain (also known as raised intracranial pressure) and a condition called brain herniation syndrome. These can include:
1. Hematoma – This is when blood collects outside the blood vessels, sometimes due to a head injury. This could be either a traumatic epidural hematoma (a bleed between the skull and outer layer of the brain), a subdural hematoma (a bleed into a space in the brain below the outermost layer), contusions (bruises on the brain), or intracerebral hemorrhage (bleeding within the brain itself).
2. Malignant infarction – this term is used when a portion of the brain dies off due to a particularly severe type of stroke.
3. Tumors – Abnormal growths in the brain.
4. Infections – These could be things like abscesses (a pocket of pus), empyema (a collection of infected fluid), or a hydatid cyst (a type of parasite).
5. Hydrocephalus – A condition where too much spinal fluid builds up inside the brain, which can cause the pressure to increase.
6. Diffuse subarachnoid hemorrhage – This is bleeding into a space between two of the membranes that cover the brain.
7. Pneumocephalus – This is a condition where there’s air or gas in the space around the brain, often due to trauma or surgery.
8. CSF overdrainage – CSF stands for cerebrospinal fluid, the clear liquid that surrounds the brain and spinal cord to protect them. Overdrainage happens when too much CSF fluid is drained, often due to a medical procedure.
9. Metabolic-hepatic encephalopathy – In this instance, confusion, altered levels of consciousness, or coma occurs due to liver failure, where the liver doesn’t effectively remove toxins from the bloodstream.
Risk Factors and Frequency for Brain Herniation
Traumatic brain injury, or TBI, is the main cause of death following a traumatic injury. Increased pressure inside the skull, or raised intracranial pressure, often leads to worse outcomes for people with a TBI.
Signs and Symptoms of Brain Herniation
Evaluating the brain function of patients with herniation, a condition where a part of the brain is squeezed into another area, requires careful attention. This includes identifying early signs of differences in pupil size and swiftly addressing the main issue to prevent further harm.
As the herniation develops, the patient may exhibit a series of neurological signs and symptoms. Here are the common ones for different types of herniation:
- Subfalcine herniation: This condition often results in weakness in the lower limbs due to blood supply interruption caused by the squeezing of blood vessels.
- Uncal herniation: It’s characterized by unequal pupil sizes on the same side as the herniation and weakness on the opposite side of the body. Sometimes, this can cause weakness on the same side as well.
- Increasing inner skull pressure: If left unchecked, this pressure can shift a part of the brain called the diencephalon, affecting awareness due to the distortion of the reticular activating system, the brain’s ‘awake’ mechanism. This also leads to a condition called hydrocephalus due to twisting and blocking of fluid paths in the brain.
- Downward transtentorial herniation: Symptoms include rigid and abnormal body posturing, loss of brainstem reflexes, and changes in breathing patterns, which can lead to no breathing at all. This often results in fixed, dilated pupils and inability to breathe due to the pressure on the breathing centers in the lower part of the brain.
- Upward transtentorial herniation: This condition triggers Parinaud syndrome, a group of eye movement disorders, and symptoms of diabetes insipidus as a result of damage to a part of the brain controlling water balance in the body.
Testing for Brain Herniation
Radiological imaging, which includes techniques like x-rays, CT scans, or MRIs, can show specific markers that are associated with different types of brain herniation.
In cases of subfalcine herniation, the imaging might show a flattening of the lateral ventricles on one side of the brain and a shifting of a thin membrane in the brain called the septum pellucidum. As this type of herniation progresses, key fluid-filled spaces in the brain, known as the basal cisterns, might show signs of compression and loss of fluid. Alongside these, there might also be increased fluid build-up in the brain, a condition known as hydrocephalus.
If there’s an uncal herniation, the imaging will show an expansion of the fluid-filled spaces in a part of the brain called the cerebellopontine cistern on one side, and the disappearance of the same spaces on the other side.
If a central herniation occurs, the images will show complete disappearance of certain critical fluid-filled spaces in the brainstem region. Alongside, there may be signs of bleeding in the brain (Duret hemorrhages).
When upward herniation happens, the image might show flattening of a part of the brain called the quadrigeminal cistern and a specific ‘spinning top’ appearance of the midbrain. This condition too might be accompanied by hydrocephalus.
The imaging can also reveal instances of stroke (infarction) in areas where blood vessels have been compressed. In advanced stages, this might present as a ‘white cerebellar sign’ indicating extensive loss of blood and oxygen to the brain.
In specific conditions, the brain’s automatic regulation of blood flow can be disturbed, making it overly responsive to changes in blood pressure. Also, the brain’s ability to adjust and compensate for changes in pressure could reduce.
Another observation in such cases could be changes in pressure waves inside the brain, specifically in the form of high, prolonged A waves and shorter, rhythmic B waves, indicating increasing pressure in the brain.
Lastly, brain herniation can also change the pattern of pressure waves within the brain as evident in the intracranial pressure (ICP) waveform, a measure of pressure within the skull. The height of the dicrotic wave, the second pressure wave in each heartbeat cycle and normally the lowest, may go above the heights of the percussion and tidal waves.
Treatment Options for Brain Herniation
Guidelines by the Brain Trauma Foundation suggest that we should monitor intracranial pressure (ICP – the pressure in your brain) in patients who have suffered severe traumatic brain injuries. The seriousness of such injuries is measured using a scale known as the Glasgow Coma Scale (GCS), with scores between 3 and 8 indicating severe injury. Monitoring is recommended when patients either have noticeable abnormalities as seen on a brain CT scan, or if they meet at least two out of three specific criteria: being over 40 years old, having low blood pressure (below 90 mmHg), or exhibiting abnormal posturing (odd positions or movements).
The reason for this method is based on the understanding that changes in brain pressure can be detected six hours before any clinical symptoms of herniation syndrome appear. Herniation syndrome is a potentially life-threatening condition where the brain shifts from its usual position due to pressure. While ICP monitoring can give key insights, different studies on this approach have given varying results.
Currently, there are no clear-cut guidelines (or level I evidence) available for the management of refractory intracranial hypertension, a condition where the pressure in the brain remains abnormally high. While we do have some moderate evidence (level IIA) supporting a surgical procedure known as decompressive hemicraniectomy and level IIB evidence supporting the use of ICP monitoring, the decisions largely depend on individual cases. For therapy guided by ICP and blood flow to the brain (cerebral perfusion pressure), the pressure levels usually aimed for are 22 mm Hg and 60 to 70 mm Hg, respectively.
The following are some proposed steps in managing persistent high brain pressure, which can lead to brain herniation:
- Removing mass lesions – this could involve removing blood clots, damaged tissue, or tumors.
- Implementing physiological neuroprotection measures to safeguard the brain.
- Administering sedation, pain relief, and ventilation to the patient.
- Draining cerebrospinal fluid to help reduce pressure.
- Using osmotherapy, a method of controlling swelling.
- Using hyperventilation to constrict blood vessels and lower pressure.
- Using hypothermia to slow brain metabolism, though this could lead to infections or abnormal heart rhythm.
- Inducing a barbiturate coma to decrease cerebral blood flow, though this could also cause low blood pressure.
- Performing decompressive hemicraniectomy, a surgical procedure where part of the skull is removed to reduce pressure.
The following general measures are also needed:
- Most patients will likely need assisted breathing (mechanical ventilation). Some patients may also need to be paralyzed to avoid straining or agitation, and sedatives can help keep them calm.
- Using controlled hyperventilation can cause blood vessels to constrict and help lower the pressure in the brain.
- Fluid intake should be carefully managed to prevent dehydration.
- Diuretic medications like mannitol can be used to help lower brain pressure.
- Controlling blood pressure is important in order to ensure the brain gets enough blood flow, but care should be taken to avoid low pressure.
- In patients with abscesses or cancer, corticosteroids can help to reduce swelling.
- While cooling the body (hypothermia) can slow brain activity, it may also make the patient more vulnerable to infections or abnormal heart rhythm.
- Inducing a coma using pentobarbital can help reduce blood flow to the brain, but it can also lead to low blood pressure.
What else can Brain Herniation be?
In some cases, a number of medical conditions could appear to be a brain herniation syndrome due their patients’ quick decline in health and neurological function. These conditions include, but are not limited to:
- Subclinical seizures after trauma
- Acute hydrocephalus (a buildup of fluid in the brain)
- Tension pneumocephalus (a buildup of air in the skull)
- Dyselectrolytemia (an imbalance of electrolytes)
- Meningitis (an infection of the protective membranes surrounding the brain and spinal chord)
- CSF over-drainage syndrome (a condition caused by the excessive drainage of cerebrospinal fluid)
- Osteopetrosis (a rare disease that makes bones overly dense)
- Costello and posterior fossa crowding syndrome (a group of rare genetic disorders)
What to expect with Brain Herniation
Several factors can affect the prognosis or outcome for a patient with a herniation, which is a condition where an organ pushes through an opening it shouldn’t. These factors include how long it’s been since the herniation started, the patient’s age, and their Glasgow coma scale score (a healthcare tool used to measure a patient’s level of consciousness, lower scores can indicate possible brain damage). Other factors include anisocoria (unequal size of the eyes’ pupils), if there are injuries in multiple parts of the body, whether there’s low oxygen or low blood pressure, and the type of brain bleed they have (extradural hemorrhage, which is bleeding between the outer layer of the brain and skull, versus subdural hemorrhage, bleeding in a specific area of the brain).
The Marshall and Rotterdam CT scores (systems used by doctors to assess brain injury) also affect the prognosis, as does the measured level of intracranial pressure (ICP), which is the pressure inside the head. If the herniation syndrome gets worse, it becomes increasingly difficult for the patient to recover.
Possible Complications When Diagnosed with Brain Herniation
Brain herniation is a serious condition that can gradually progress through different stages, each with unique symptoms. It can start with uneven pupils (a condition called uncal herniation) and progress to altered consciousness, indicated by the inability of maintain wakefulness or attention (due to pressure on the reticular activating system). This can worsen to abnormal body postures due to compression of the diencephalon and the brainstem, and ultimately, can lead to death as a result of respiratory failure caused by pressure on the medulla, a part of the brainstem that controls breathing.
In addition to these symptoms, brain herniation can also lead to blockages in the blood supply to different areas of the brain, leading to tissue death, a condition referred to as brain infarction. Each type of herniation affects specific blood vessels and their associated regions in the brain. In the final stages, this brain tissue death can be widespread. In fact, a non-contrast CT scan of the brain can visually highlight these infarctions, as evidenced by a “white cerebellar sign.”
Main progressions to note:
- Uneven pupils (uncal herniation)
- Altered level of consciousness
- Abnormal body postures
- Death resulting from respiratory failure
- Brain tissue death from blocked blood supply
- Radiological evidence of widespread brain tissue death
Preventing Brain Herniation
The main way to prevent head injuries is by making people aware of the importance of following traffic rules, wearing helmets while riding bikes, always using seat belts in cars, and not driving when drunk. This knowledge can help to reduce the risk of head injuries.











